Download

1 / 56
600 likes | 828 Views
Fever and Rash. Dr. Orli Megged Infectious Diseases Unit Shaare Zedek Medical Center. How do you describe this rash?. Multiple erythematous macules and/or papules, a few millimeters to 1 cm in size. Symmetric distribution on trunk and extremities. Dermatologic Terminology. Macule Papule

E N D
Fever and Rash Dr. Orli Megged Infectious Diseases Unit Shaare Zedek Medical Center
How do you describe this rash? Multiple erythematous macules and/or papules, a few millimeters to 1 cm in size. Symmetric distribution on trunk and extremities
Dermatologic Terminology • Macule • Papule • Nodule • Vesicle • Bulla • Pustule • Petechia • Purpura • Ecchymoses • Erythroderma
Macule Flat, nonpalpable circumscribed area of change in the skin color, may be any size.
Papule Solid raised skin lesion with a distinct borders, generally < 5 mm in diameter.
Nodule Palpable, solid, round, or ellipsoidal lesion > 5 mm diameter
Vesicle (blister) Circumscribed, elevated lesion that is < 5 mm in diameter containing serous (clear) fluid.
Bulla A vesicle with a diameter > 5 mm.
Pustule Superficial, elevated lesion that contains pus.
Petechia A small (1-2mm) red or purple discolorations on the skin, caused by a minor hemorrhage (do not blanch on applying pressure)
Purpura 0.3-1 cm.
Ecchymoses Greater than 1 cm.
Erythroderma Erythema that affects nearly the entire cutaneous surface (“red man”)
Describing rash • Color • Margination • Shape • Palpation • Number • Arrangement - Generalized, Symmetric, Flexural, Extensor, Palmoplantar, Photo-distributed • Confluence
Asking the right questions • Site of onset, rate & direction of spread. • Distribution, configuration and arrangement of the lesion? • Is there erythema, hypo, or hyperpigmentation? • Are there secondary characteristics such as scale? • Is pruritus present? • Is the patient taking any meds (prescription, OTC, herbal) • Travel History? • Immune Status?
DD bullous rash • Viral • Bacterial • Drugs • Allergic Contact Dermatitis • Autoimmune blistering diseases of the skin • ….
Varicella – Chicken Pox Varicella Zoster Virus • Incubation period: 10 – 21 days • Infectious: 2d prior to rash – 5d after • Vaccinations – live attenuated: • Varilrix • MMRV
DD bullous rash • Bacterial
DD petechial/pupuric rash • Meningococcal disease • Rickettsial infection • Endocarditis • Sepsis • Viral (enterovirus) • Viral hemorrhagic fevers • “Noninfectious” TTP, HSP, vasculitis, etc.
Meningococcemia • Neisseriameningitidis • Gram-negative diplococci • Strains are grouped based on a polysaccharide capsule • A, B, C, Y and W135
Meningococcemia • Petechial rash • With or without meningitis • Case fatality rate is between 8-15%
Rickettsia Conorii • Intracellular, slow-growing gram-negative bacterium • Mediterranean spotted fever (MSF) • Common dog tick is the vector in the Mediterranean.
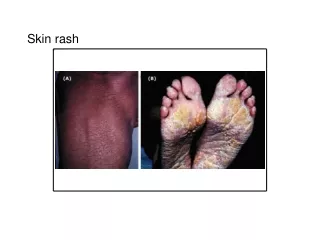
Spotted fever • Incubation 2-14 days, median 7 days • Fever, myalgia, headache, GI • Rash - typically begins around the wrists and ankles. • Involvement of the palms and soles - characteristic
HSP • Systemic vasulitis, palpable purpura • Deposition of immune complexes containing IgA • Mainly in children • Symptoms: joint & abdominal pain • Complications: irreversible kidney damage
DD: Maculo Papular rash • Viral • Bacterial • Other Infections: Secondary Syphilis, Lyme • Kawasaki’s • Drugs • Rheum: SLE, Reiter’s Syndrome
Viral • Measles • Rubella • Parvo • EBV • CMV • HHV6 • Adeno • Entero • WNF
Bacterial • Strep pyogenes (Scarlet Fever) • Staph aureus (TSS) • Meningococcemia • Spotted fever
This teenager was referred by his family physician for neurological assessment • Name the clinical feature • Right facial nerve palsy of lower motor neuron type • What is the diagnosis? • Ramsay-Hunt syndrome • What is the causative organism? • Varicella-zoster virus • What is the long-term prognosis? • Facial paralysis may be permanent
A 12-year-old epileptic boy, developed fever, dry cough and tachypnoea. He was seen by a family physician, who prescribed symptomatic treatment and a course of antibiotics. A generalized skin rash appeared 2 days afterwards What is the clinical feature? Erythema multiforme What are the possible etiologies? • Drugs e.g. carbamazepine, phenobarbitone • Infections e.g. herpes simplex, mycoplasma or streptococcus • Idiopathic
Several pupils of a kindergarten were seen because of acute onset of fever, itchy skin lesions at the extremities and sore throat. • Name the diagnosis • Hand, foot and mouth disease • What is the most likely causative organism? • Usually Coxsackievirus A16 or Enterovirus 71 • Complications? • Aseptic meningitis. Enterovirus 71 may cause meningoencephalitis or polio-like acute flaccid paralysis
6-month-old infant with vesicular skin lesions, distributed on the area corresponding to the L3 dermatome. • What is the diagnosis? • Herpes zoster • The infant did not have a history of chickenpox before. What further information would you ask? • Maternal chickenpox during pregnancy • What is the prognosis? • Possible recurrent herpes zoster during infancy
A 2-year-old child with fever, vomiting, diarrhea, conjunctival injection and rapidly spreading generalized erythema . The BP was not recordable. He developed acute renal failure and ARDS.
What is the clinical feature of the face and trunk? • Erythroderma • What is your presumptive diagnosis? • Toxic shock syndrome • What is the likely causative organism? • Staphylococcus aureus, Streptococcus pyogenes • What is the current proposed pathogenesis of the condition? • T cell activation by toxins behaving as superantigens, TSST-1