Download
1 / 27
280 likes | 606 Views
MALIGNANT HYPERTHERMIA. Dr. Mary Lehane Malignant Hyperthermia Investigation Unit Cork University Hospital. INCIDENCE. 1:12 000 - 1:40 000 Male = Female No racial difference. MORTALITY. 5 % - 80 %. TRIGGERS. All volatile anaesthetic agents Suxamethonium. GENETICS.

E N D
MALIGNANT HYPERTHERMIA Dr. Mary Lehane Malignant Hyperthermia Investigation Unit Cork University Hospital
INCIDENCE • 1:12 000 - 1:40 000 • Male = Female • No racial difference
MORTALITY 5 % - 80 %
TRIGGERS • All volatile anaesthetic agents • Suxamethonium
GENETICS • Autosomal dominant • Chromosome 19 • Gene RYR 1 • Mutations • 78 single point mutations identified to date
PRESENTATION • 1 A known MH patient • 2 Unexpected MH crisis
FULMINANT CRISIS • Tachycardia • Metabolic acidosis, O2 sat, pCO2 • Muscle rigidity • Electrolyte disturbance • Arrhythmias • Myoglobinuria • Hyperthermia
DIAGNOSIS, consider MH if • Masseter muscle spasm after sux • Unexplained, unexpected tachycardia • Unexplained, unexpected increase in end - tidal CO2
EARLY MANAGEMENT 1 • STOP ALL ANAESTHETIC VAPOURS • CHANGE TO CLEAN ANAESTHETIC BREATHING SYSTEM • ABANDON SURGERY IF FEASABLE
EARLY MANAGEMENT 2 • DANTROLENE • MEASURE ABGs, K+ AND CK • MEASURE CORE TEMP • COOL PATIENT
OTHER COMPLICATIONS • Arrhythmias • Hyperkalaemia • Metabolic Acidosis • Disseminated Intravascular Coagulopathy • Renal Failure
POST CRISIS MANAGEMENT • WARN PATIENT AND FAMILY • REFER FOR INVESTIGATION • ie muscle biopsy • MEDIC ALERT
INVESTIGATION • Family history • Muscle biopsy • In - vitro contracture tests • Histology • Resting CPK etc • Mutation screening
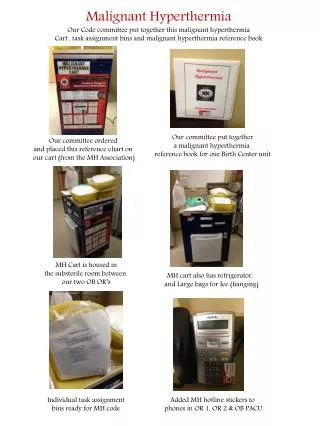
KNOWN MH PATIENT • Inform anaesthetist and theatre • Prepare anaesthetic machine etc • All hospitals should carry dantrolene • All staff carry responsibility
The Cork Experience • 560 Patients biopsied • MHS 131 • MHE (h) 100 • MHE (c) 6 • MHN 333
The Cork Families • 98 Pedigrees identified • 74 Probands • 24 Deaths
CONCLUSION • SURVIVAL • Identification of at-risk patients • Appropriate management