Download
1 / 37
381 likes | 477 Views
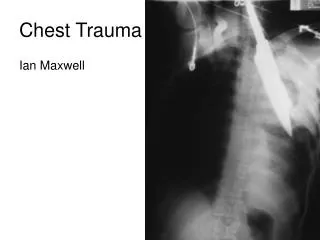
Chest Film Primer Images and Material courtesy of:. David S. Feigin, M.D. Colonel (Ret), USA, MC Professor of Radiology, Uniformed Services University of the Health Sciences “A Systematic Approach To Abnormal Chest Images: Radiographs And Computed Tomograms” Updates and compilation:

E N D
Chest Film PrimerImages and Material courtesy of: David S. Feigin, M.D. Colonel (Ret), USA, MC Professor of Radiology, Uniformed Services University of the Health Sciences “A Systematic Approach To Abnormal Chest Images:Radiographs And Computed Tomograms” Updates and compilation: Les Folio, DO, MPH Col, USAF, MC, SFS Associate Professor of Radiology, Uniformed Services University of the Health Sciences
EXIT Main Menu • NORMAL ANATOMY • A-P Chest Radiograph • Lateral Chest Radiograph • 5 PATTERNS OF PATHOLOGY • Mass • Consolidative • Interstitial • Linear • Nodular • Vascular • Airway • Wall-Thickened • Obstructive • THE SEARCH PATTERN • A-P Chest Radiograph • Lateral Chest Radiograph
BACK MAIN MENUFORWARD Normal Anatomy- AP 1. Gross Specimen 2. The Respiratory System A. The Airway B. The Lungs and Diaphragm • Cardiovascular System • A. The Cavals B. The Heart SVC Edge Left paratracheal stripe LUL C. The Pulmonary Arteries RUL, next to minor fissure D. The Pulmonary Veins E. Aorta 3. The Bones, Bowel Gas, Azygous, etc. Right Atrium Left Ventricle RML, next to right heart border RLL LLL
BACK MAIN MENUFORWARD Normal Anatomy- Lateral 1. Respiratory System A. The Airway B. The Lungs and Diaphragm RUL Trachea 2. Cardiovascular System Aorta A. The Vessels Right Pulmonary Artery B. The Heart Left Pulmonary Artery Left main bronchus RML, with minor fissure 3. The Bones (no link yet) Right Ventricle RLL, with major fissure Left Ventricle Inferior Vena Cava
Quiz yourself: Mediastinum Lines, Edges Recommendation: Test yourself before advancing to the answers • SVC Edge • Rt Paratracheal Line • Lt Paratracheal Stripe (both red and black lines) • Aortic Arch • Descending Aorta (only left edge seen, and not always) • Rt Atrium • Azygoesophageal edge • Lt Ventricle • Main Pulmonary Artery AKA: trunk, middle mogul 3 1 2 4 9 5 6 7 8 Mediastinum Mid
Trachea Lt MSB on end Right Pulmonary Artery (red) Left Pulmonary Artery (green) Left Ventricle (curved line) IVC (arrows) Lateral
EXIT Main Menu • NORMAL ANATOMY • A-P Chest Radiograph • Lateral Chest Radiograph • The 5 PATTERNS OF PATHOLOGY • Mass • Consolidative • Interstitial • Linear • Nodular • Vascular • Airway • Wall-Thickened • Obstructive • THE SEARCH PATTERN • A-P Chest Radiograph • Lateral Chest Radiograph
BACK MAIN MENUFORWARD Search Pattern- AP PRELIMINARIES Verify patient info, date, L and R markers Note technique deficiencies Quick look at both films for obvious abnormalities FRONTAL 1. LUNGS Up and down Side to side Volume and Symmetry 2. PERIPHERY Pneumothorax (air) Effusions (fluid) 3. MEDIASTINUM Contours Edges Shape 4. TRACHEA AND MAIN BRONCHI 5. HILA Enlargement Abnormal bulges 6. PERIPHERY OF CHEST Neck Chest wall and bones Diaphragms Upper abdomen
BACK MAIN MENUFORWARD Search Pattern- Lateral PRELIMINARIES Verify patient info, date, L and R markers Note technique deficiencies Quick look at both films for obvious abnormalities LATERAL 1. SIZE AND SHAPE OF LUNGS AND DIAPHRAGMS 2. AIRWAY Neck to Hilum Pulmonary Arteries 3. Back of heart and darkening downward 4. Up anterior mediastinum for darkening 5. Down spine for vertebral bodies and darkening 6. PERIPHERY Abdomen Anterior chest wall Posterior ribs Costophrenic angles
EXIT Main Menu • NORMAL ANATOMY • A-P Chest Radiograph • Lateral Chest Radiograph • 5 PATTERNS OF PATHOLOGY • Mass • Consolidative • Interstitial • Linear • Nodular • Vascular • Airway • Wall-Thickened • Obstructive • THE SEARCH PATTERN • A-P Chest Radiograph • Lateral Chest Radiograph
BACK MAIN MENUFORWARD 1. Mass • Mechanism - Local destruction of lung parenchyma • Radiological sign - Any localized opacity not completely bordered by fissures or pleura
BACK MAIN MENUFORWARD 1. Mass • Differential Diagnosis • Malignancy - Primary or secondary • Granulomatous disease - Infectious or noninfectious, active or inactive • Other inflammation, including pneumonia and abscess, Benign neoplasm, Congenital abnormality • Crucial appearance characteristics for inactivity • Calcification – central, lamellar • Evolution – 2-year stability or regression
BACK MAIN MENUFORWARD 2. Consolidative (Alveolar) Pattern • Mechanism • Produced in pure form and by ALVEOLAR FILLING • May be mimicked by alveolar collapse, as in airway obstruction • Rarely, confluent interstitial thickening • Radiological signs • Fluffy, cloud-like, coalescent opacities • Sharp edges when limited by fissures or pleura • Complete air bronchograms through the clouds
BACK MAIN MENUFORWARD Fluffy and cloud-like appearance Air bronchograms THROUGH clouds
BACK MAIN MENUFORWARD Air bronchogram Normal lung Consolidated lung, with air in bronchioles
BACK MAIN MENUFORWARD 2. Consolidative (alveolar) Pattern • Differential Diagnosis (5 general) • Hemorrhage - BLOOD - embolism, trauma • Exudate - PUS - pneumonia, pneumonitis • Transudate - WATER - congestion, ARDS • Secretions - PROTEIN - Mucous plugging, Alveolar proteinosis • Malignancy - CELLS - Alveolar cell carcinoma, Lymphoma
BACK MAIN MENUFORWARD 3. Interstitial Pattern • Composition of pulmonary interstitium: • Alveolar walls, septi • Connective tissue surrounding bronchi and vessels (peribronchial and perivascular spaces) • Mechanism • Thickening of lung interstices • Architectural destruction of interstitium (honeycomb or “end stage” lung)
BACK MAIN MENUFORWARD 3. Interstitial Pattern • Radiological Signs: • Linear form - reticulations (lines in all directions), septal lines (Kerley lines) • Nodular form - small, sharp, numerous, evenly distributed, uniform (especially uniform in shape) nodules • Destructive form - peripheral, irregular cyst formation
BACK MAIN MENUFORWARD 3. Interstitial Pattern • Radiological Signs: • Linear form - reticulations (lines in all directions), septal lines (Kerley lines) • Nodular form - small, sharp, numerous, evenly distributed, uniform (especially uniform in shape) nodules • Destructive form - peripheral, irregular cyst formation
BACK MAIN MENUFORWARD Kerley B lines (horizontal septal) Reticular form (Lines in all directions)
BACK MAIN MENUFORWARD 3. Interstitial Pattern – Linear Form • Differential Diagnosis: The “LIFE Lines” • Lymphangitic spread of malignancy • Inflammation • Fibrosis • Edema
BACK MAIN MENUFORWARD 3. Interstitial Pattern • Radiological Signs: • Linear form - reticulations (lines in all directions), septal lines (Kerley lines) • Nodular form - small, sharp, numerous, evenly distributed, uniform (especially uniform in shape) nodules • Destructive form - peripheral, irregular cyst formation
BACK MAIN MENUFORWARD Multiple small nodules, uniform in shape and distribution
BACK MAIN MENUFORWARD 3. Interstitial Pattern- Nodular Form Granulomatous Diseases: Infectious Tuberculosis Atypical mycobacterial diseases - especially MAI Fungal diseases, especially: Histoplasmosis Coccidioidomycosis Blastomycosis (N. A. and S. A.) Cryptococcosis Sporotrichosis Bacterial diseases, especially: Nocardiosis Actinomycosis Non-infectious Sarcoidosis Hypersensitivity Pneumonitis (HP) Vasculitis-granulomatosis diseases Wegener’s Lymphocytic Bronchocentric Allergic (Churg-Strauss) Langerhans Granulomatosis (eosinophilic granuloma, histiocytosis) (LCG) • Differential Diagnosis Pneumoconiousus Granulomatous Silicosis Berylliosis “Benign” Coal Worker’s Pneumoconiosis Siderosis Stannosis 1. Granulomas 2. Hematogenous Spread of Malignancy 3. Pneumoconiosus
BACK MAIN MENUFORWARD 3. Interstitial Pattern • Radiological Signs: • Linear form - reticulations (lines in all directions), septal lines (Kerley lines) • Nodular form - small, sharp, numerous, evenly distributed, uniform (especially uniform in shape) nodules • Destructive form - peripheral, irregular cyst formation
BACK MAIN MENUFORWARD Early findings are non-specific. The peripheral cyst formation (“End-Stage Lung”) is a late finding. Peripheral cyst formation, ‘Honeycomb’ lung
BACK MAIN MENUFORWARD 4. Vascular Patterns • Mechanism - increased, or decreasedperfusion, altering diameter of pulmonaryvessels • Radiological signs - changes in diameterof specific vessels
BACK MAIN MENUFORWARD 4. Vascular Patterns • Common examples • Congestion- engorged veins, especially upper lungs • Emphysema- diminished vessels • Shunt vascularity - all vessels enlarged • Lymphangitic carcinoma - irregular infiltration around vessels may resemble vessel enlargement • Arterial hypertension- large central arteries with peripheral tapering • Thromboembolism - locally diminished vessels with possible vessel mass centrally located • Bronchial circulation - irregular vessels in unusual directions
BACK MAIN MENUFORWARD Engorged vessels, especially upper lungs Congested vasculature
BACK MAIN MENUFORWARD Diminished vasculature Emphysematous changes
BACK MAIN MENUFORWARD Enlarged pulmonary trunk (“middle mogul”) Prominent left pulmonary artery
BACK MAIN MENUFORWARD 5. Airway (Bronchial) Patterns • Mechanism • Complete or partial obstruction of airways • Thickening of airway walls • Forms • Complete airway obstruction - opacity and decreased volume • Partial obstruction - lucency and increased volume • Wall thickening - tram tracks, central cystic spaces or circles
BACK MAIN MENUFORWARD Flattened diaphragms on lateral Bronchial wall thickening (circles and “tram tracks”)
BACK MAIN MENU FORWARD 5. Airway (Bronchial) Patterns • Differential diagnosis • Opacities - endobronchial malignancies, granulomas, inflammatory, benign or congenital masses, mucous plugs, foreign bodies • Lucencies - COPD, cysts, blebs, pneumatoceles • Thickening - bronchiectasis, chronic bronchitis
BACK MAIN MENU FORWARD 5. Airway (Bronchial) Patterns • Lobar atelectasis (collapse) • Primary Signs • Vessel number assymetry • Fissure as edge • Secondary signs • Volume loss • Elevation of diaphragm • Shift of mediastinum and ribs
Atelectasis Patterns Right Left Upper RUL LUL Lower LLL RLL
BACK MAIN MENU EXIT Vessel Asymmetry Left lower lung collapse