Download
1 / 45
450 likes | 545 Views
Strategizing for Accountable Care. Medical Society of Northern Virginia March 29, 2011 MIKE NEWBY MARY MALONE HANCOCK, DANIEL, JOHNSON & NAGLE, PC. Presentation Overview. What is an ACO? LLC Formation and Governance Medicare’s Shared Savings Program Legal Issues

E N D
Strategizing for Accountable Care Medical Society of Northern Virginia March 29, 2011 MIKE NEWBY MARY MALONE HANCOCK, DANIEL, JOHNSON & NAGLE, PC
Presentation Overview • What is an ACO? • LLC Formation and Governance • Medicare’s Shared Savings Program • Legal Issues • How to Position Yourself for Accountable Care • Q&A
An ACO is an entity that is clinically and fiscally accountable for the entire continuum of care that a given population of patients may need Focus of presentation is on the Medicare ACO opportunity, though “ACO-like” options are being discussed with health plans as well What is an ACO?
Three Principles: Provider led organizations with a strong base of primary care that are collectively accountable for quality and total per capita costs across the full continuum of care for a defined patient population Link payment to quality improvements to reduce overall costs Evidenced-based medicine What is an ACO?
What is an ACO? Financial pressures creating shift in reimbursement strategy Movement away from fee-for-service payment methodology. Current system promotes high-volume and high-intensity health services, regardless of quality and whether care is coordinated. Emphasis on quality, efficiency and coordinated care.
What is an ACO? ACOs incorporate ideas of other models: • Physician-hospital organizations (PHOs) • Integrated delivery systems • Independent provider associations (IPAs) • Hospital employment of physicians
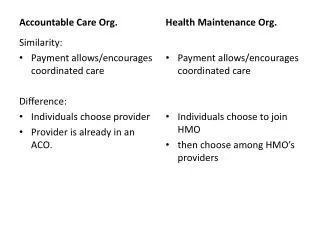
Is This Déjà Vu All Over Again? Historical Managed Care Focus on Insurers, HMOs Reliance on health plan intermediaries Shared financial risk; insurance regulation Beneficiaries required to enroll in particular plan, use only particular providers ACOs Focus on delivery system Direct contracting with delivery organizations Potential for upside only sharing Beneficiaries assigned by primary care usage and may change ACOs at will Greater flexibility: Variety of eligible providers and models Variety in payment methodology
LLC Formation and Governance Initial Steps: • File Articles of Organization • Obtain EIN • Enact Operating Agreement and organizational resolutions • Register with VEC and the Virginia Department of Taxation • Obtain a Business License
LLC Formation and Governance Operating Agreement – Investment and Management • Capital Contributions (seed money) • Management by members or managers • Appointment of managers • Authority of managers • Capital calls • Distributions
LLC Formation and Governance Operating Agreement – Members Rights • Sale/acquisition of property over a certain dollar amount • Starting new business activities or entering in new contracts • Leases with minimum durations • Borrowing money • Requesting capital contributions • Admission of new members
LLC Formation and Governance Operating Agreement – Other Issues • Withdrawal • Admission of new members • Purchase/redemption price • Restrictive covenants • Fiduciary duties • Confidentiality • Conflicts and deadlock
LLC Formation and Governance Attributes: • Pass-through taxation • Limited liability • Flexible • Best approach for ACOs? Stay Tuned.
Medicare’s Shared Savings Program • Effective January 1, 2012 • Goals • Investment in infrastructure • Redesign of care process – patient focused • Quality and efficiency • Medicare Parts A and B (not parts C & D) • Serves traditional Medicare beneficiaries
Medicare’s Shared Savings Program Characteristics of an ACO: • Emphasis on evidence-based clinical care • Close monitoring and reporting of quality and cost savings • Coordinated care: clinical protocols / EHR • No beneficiary network restrictions • Does CMS contract mean “certification”?
Medicare’s Shared Savings ProgramUpside-only Model Projected Spending Target Spending Shared Savings Actual Spending -3 -2 -1 0 1 2 3 Year Source: Dartmouth Institute for Health Policy and Clinical Practice
Medicare’s Shared Savings Program Providers - ACO must be big enough so that cost savings can be tied to quality improvements and not year-to-year fluctuations in care • Equity participants • Contractors At least 5,000 Medicare beneficiaries according to the Medicare Payment Advisory Commission • Approx. 5-6 PCPs per 5,000
Medicare’s Shared Savings Program Need for formal organization and designated administrator • Point of contact • Ability to work with and negotiate with payors • Monitor performance and shared savings • Development and implementation of strategies and infrastructure to coordinate care
Accountable Care Organizations Approaches to Reimbursement Goal: Reward strong clinical performance and efficiency through: • Shared savings • Capitation / Bundling • P4P / Gainsharing
Primary Legal Issues Related to ACO Formation • Antitrust Issues • Lessen competition • Conspiracy to fix prices • Unreasonable restraints of trade • Stark / CMP / Antikickback • Waivers • But watch out for state law
Antitrust Issues Related to Network Formation Integrated vs. Non-Integrated Models Types of Integration: • Clinical Integration • Financial Integration • FTC: Agreements between competing physicians, or other health care providers, on the prices to be charged for their individual services are agreements in restraint of competition and are generally illegal, absent a showing of substantial financial or clinical integration. • If integrated single signature contracting
Antitrust Issues Related to Network Formation Use Messenger Model if No Integration Allows network contracting withhealth insurance plans without collective negotiation The Messenger: • Serves as an intermediary between the payor and the physician on rates and competitive issues • May share objective factual information with providers about the payor and its business • May negotiate non-competitive terms • May not negotiate rates or competitive terms • May not serve as an advocate on rates or share competitive information
Antitrust Issues Related to Network FormationMedSouth Advisory Opinion Background • Multi-specialty IPA consisting of 432 physicians (101 primary care/ 331 specialists) in Denver area covering 3 hospitals • Non-exclusive, but covered more than 50% of the physicians in over 20 practice areas at 3 area hospitals • Clinical protocols covering 80%-90% of diagnosis • 48 established as of date of opinion; additional 100-150 protocols contemplated • Utilization and quality measured against protocols • Clinical Information System to monitor quality measures • Ability to discipline non-complying physicians • Web-Based Clinical Data System • Online prescriptions
Antitrust Issues Related to Network FormationMedSouth Advisory Opinion • Purposes: improved patient care and outcomes, reduction in medical errors, increased efficiency, reduction in costs, ability to discipline and terminate sub-standard physicians • Conclusion: Substantial likelihood of achieving efficiencies outweighed anti-competitive effects
Antitrust Issues Related to Network Formation FTC’s Gloss on Clinical Integration • Integration of institutions and practitioners that presents the opportunity for true collaboration and productive sharing of information reflecting actual “interdependence” • Participation of both specialists and primary care physicians with a requirement of in-network referrals • Treatment of a broad spectrum of diseases and disorders and corresponding clinical protocols • A high level of physician investment, both economically and in terms of time for training and utilization of the system, and agreement among physicians to comply with the standards, benchmarks, and protocols put in place by the network
Antitrust Issues Related to Network Formation FTC’s Gloss on Clinical Integration (Continued) • Integrated information technology whereby: • network participants can efficiently exchange information regarding patients and practice experience • utilization and claims information can be gathered, analyzed, and communicated in order to improve treatment quality, rates of utilization, and cost containment • physician compliance and performance, in accordance with collective, physician-authored benchmarks and standards, may be measured • Enforceable consequences for noncompliance by physicians and institutions, and systems for improving performance and compliance
Legal Issues - Takeaways Antitrust: ACO Network formation may implicate antitrust laws, but integrated approach can mitigate risk. Stark: currently no clear mechanisms for distributing shared savings, but may present opportunities with commercial payors CMP: can’t pay to reduce services, but favorable guidance for quality and efficiency based compensation especially when operating in the commercial market
How to Position Yourself Building an Infrastructure • Leadership and Vision • Engaged Provider Network • Network Formation and Formalized Legal Structure • IT infrastructure and clinical benchmarking • Effective Medical Management • Capital to Fund Development and Cash Flow • Risk Management
How to Position Yourself Develop Leadership and Vision • Identify strategically important, high performing physicians who are committed to organizational goals Develop Engaged Provider Network • Expand management and governance roles of physicians
How to Position Yourself Create a network with a formalized legal structure • Capable of distributing shared savings • Significant physician involvement in governance • Platform for clinical integration, joint contracting, information sharing
How to Position Yourself Implement Health Information Technology • Benchmarking and quality improvement as conditions of participation • Consent to share information • Can use Stark exception to subsidize up to 85% of EHR for physicians • Eligibility for federal programs (and avoidance of penalties when programs like PQRI become mandatory) may be conditioned on having information technology
How to Position Yourself HITECH Act: A Carrot and Stick Approach to Adoption and Meaningful Use of HIT
How to Position Yourself Physician Quality Reporting Initiative (PQRI) Started in 2007 as an incentive program to encourage data reporting Affordable Care Act renamed to PQRS Bonus payments for quality reporting by “eligible professionals”: 1% in 2011 and .5% in 2012 through 2014. But beginning 2015, EPs who fail to meet reporting requirements will see a 1.5% reduction in Medicare reimbursement
How to Position Yourself Financial Incentives for Adoption of ePrescribing Technology under Medicare Improvements for Patients and Providers Act of 2008 Incentive payments and penalties to eligible professionals when they ePrescribe for Medicare patients seen in their offices Carve our from PQRI program
How to Position Yourself Peer Review and PSO • Peer review to enforce quality standards applicable to the ACO and individual participants • Virginia law permits sharing of peer review information among peer review bodies • PSO to aggregate and analyze data, establish benchmarks, conduct educational programs and corrective action plans
How to Position Yourself P4P and Gainsharing • Implement compensation structure that rewards participants for quality and efficiency Additional Add-On Features • MSO, Joint Purchasing, Risk Purchasing Group, Clinical Co-Management, Professional Employer Organization, Recruitment Assistance, CME, Credentialing Verification Organization, etc.
How to Position Yourself Capital to Fund Development and Cash Flow • Secure seed money in advance Risk Management • Limit risk through incremental, small pilots • Test models through controlled models, such as an owned health plan or an insured employee base • Prepare exit strategy if experiments do not go as planned
Soon to be revealed . . . How will the rewards be structured? How will beneficiaries be assigned? How burdensome will Medicare reporting requirements be? Will there be regulatory relief on Stark and Anti-kickback to facilitate shared savings with physicians? • How many ACOs will be approved initially; what about subsequent rounds?
Next Steps: • Identify the key facilitators • Set goals and expectations • EHR • Develop protocols and benchmarks • Structure, administration, leadership, financing • Timeline • Meet with commercial payors • Evaluate strengths and weaknesses • Evaluate horizontal and vertical alliances
Mike Newby Mary Malone Hancock, Daniel, Johnson & Nagle, P.C. P.O. Box 72050 Richmond, VA 23255 804-967-9604 mnewby@hdjn.com mmalone@hdjn.com