Download
1 / 26
980 likes | 4.31k Views
Allergy Testing. Melisa Steele, CPNP Intermountain Healthcare Memorial Clinic Allergy and Asthma Department September 21, 2012. Objectives. Discuss who needs to be allergy tested and when to perform testing Summarize allergy testing guidelines

E N D
Allergy Testing Melisa Steele, CPNP Intermountain Healthcare Memorial Clinic Allergy and Asthma Department September 21, 2012
Objectives • Discuss who needs to be allergy tested and when to perform testing • Summarize allergy testing guidelines • Identify acceptable methods of allergy testing
Testing done in an Allergy Office • Food Allergy Tests • Milk, Egg, Wheat, Soy • Fish, Shellfish, Peanuts, Tree nuts • Fresh Fruits and Vegetables • Other foods as needed • Seasonal and Perennial Allergy Tests • Pollen, Dust Mites, Mold and Animals • Oral Food Challenges • Bee Venom Allergy Tests • Antibiotic Allergy Tests
At what age can you expect allergies? • Food allergy • Any age, typically start testing patients after 6 months of age • Perennial Allergies (animals, dust mites, mold) • Starts as young as 6 months • Seasonal Allergies • Earliest-age 2 • Not common before age 4
Types of adverse reactions to food • Source: Journal of Allergy and Clinical Immunology 2010; 126:S1-S58 (DOI:10.1016/j.jaci.2010.10.007 )
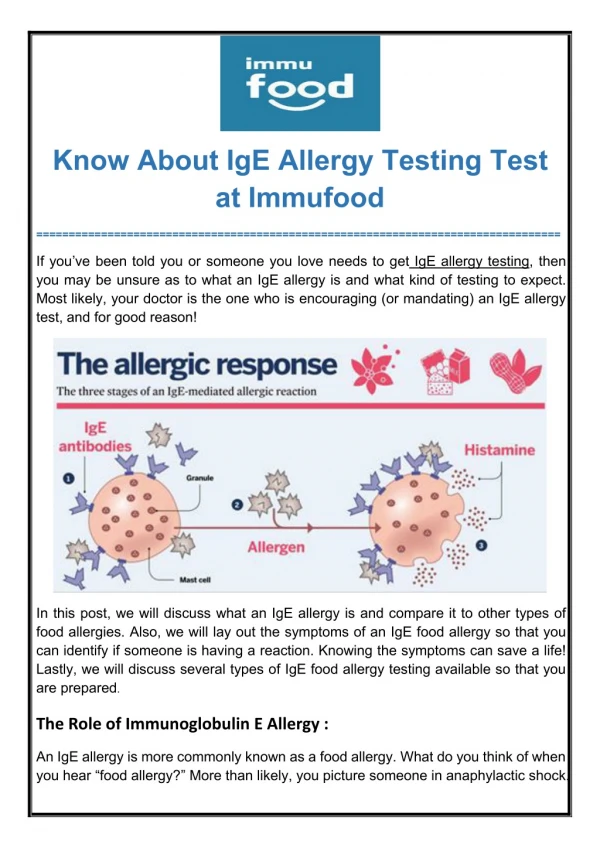
How is IgE related to allergic reactions? • IgE mediated reaction: • Your body misinterprets an antigen (food, pollen, animal, venom) it is exposed to and makes IgE (antibody) to protect itself. • IgE then attaches to floating mast cells/basophils. • The next time the antigen appears, it binds to the IgE • This triggers the attached mast cell to release chemicals that cause allergic symptoms (skin, respiratory, GI, anaphylaxis.)
Common IgE-mediated Food Allergy Symptoms • Cutaneous • Acute urticaria and angioedema • Erythema • Pruritus • Atopic dermatitis • Respiratory • Nasal congestion • Laryngeal edema • Cough • Dyspnea • wheezing • Cardiovascular • Tachycardia • Hypotension • Dizziness • Fainting • Gastrointestinal • Angioedema of the lips, tongue or palate • Oral pruritus • Tongue swelling • Nausea • Abdominal pain • Vomiting • Diarrhea • Miscellaneous • Uterine contractions • Sense of “impending doom”
What do you need to know about food allergies? • 95% of food allergies are caused by the 8 main food allergens • milk, egg, wheat, soy, peanut, tree nut, fish and shellfish. • Food allergy is more common in children than adults • 6-8% of children under age 5. • Most food allergies appear within the first 2 years of life although peanut, tree nut and seafood allergies may begin at any age. • Milk, egg, wheat and soy allergies usually resolve in childhood. • Peanut, tree nut, fish/shellfish are more likely to persist. • Food allergy that starts in adult life tends to persist. • Allergy to sesame seed is becoming more common.
Need to know continued: • About half of individuals with a food allergy will react to more than one food. • No diagnostic testing is available to predict severity of future reactions. • Risk factors for the development of food allergy: • Family history of atopy • Presence of atopic dermatitis, especially moderate to severe AD, in children under the age of 5
When should food allergy be suspected or who needs to be tested? • In individuals presenting with anaphylaxis or with typical symptoms (e.g. urticaria, edema, wheezing, mouth itch, cough, nausea/vomiting, etc.) • occurs within minutes to hours of ingesting food, • especially in young children • if symptoms have followed the ingestion of a specific food on more than 1 occasion • Children and adults diagnosed with certain disorders • Eosinophilic esophagitis, enterocolitis, enteropathy, and allergic proctocolitis • Children less than 5 years old with persistent atopic dermatitis in spite of optimized management and topical therapy • 30-40% will have food allergy
Things to Know Before Sending a Patient for Allergy Testing • All antihistamines must be stopped 7 days prior to testing. • Tricyclic antidepressants should be stopped 10 days before testing but only under the direct supervision of the prescribing physician and should not be abruptly terminated. • H2 blockers may suppress test results and might need to be stopped as well. Don’t stop unless instructed at first visit. • Patient should bring any pertinent studies or results with them (chest or sinus CT scans, xrays, copies of previous allergy testing, list of current medications, etc). • The first visit can last 2-2 ½ hours.
Food Allergy Evaluation • Detailed history: • List of suspected foods • Quantity of food eliciting a reaction • Reproducibility of reaction • Time between exposure and reactions • Clinical manifestations • Resolution of symptoms with elimination of the suspect food • Treatment given and overall duration of symptoms after each exposure • Physical Exam • Focus on suspected target organ systems (cutaneous, respiratory, gastrointestinal)
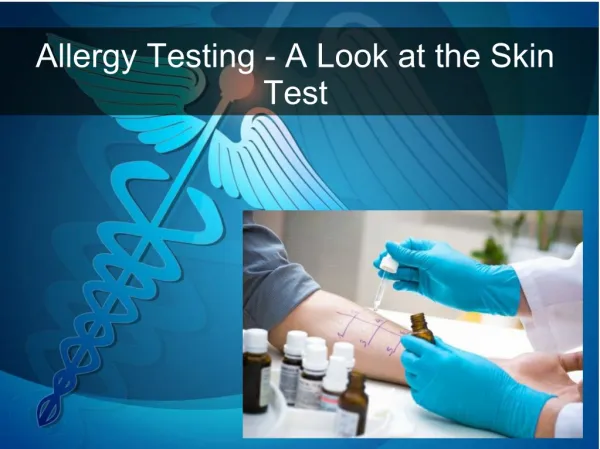
Food Allergy Evaluation • Skin prick test/Skin puncture test (SPT) • Safe and useful for identifying foods potentially provoking IgE-mediated food-induced allergic reactions • SPT alone cannot be considered diagnostic of food allergy • Testing is done on the lower arm or back • Always place a positive histamine control and a negative saline control • Wheals and flares are measured in millimeters
Food Allergy Evaluation • Skin prick test/Skin puncture test (SPT) • Positive SPT is considered a wheal 3mm greater than the negative control • Positive SPT only indicates presence of IgE antibody, NOT clinical reactivity (~50% false positive) therefore NOT a good screening tool • Negative SPT essentially excludes IgE antibody (>95%) • Results are “immediate”, typically within 15 minutes following the SPT • Intradermal tests should not be used
Food Allergy Evaluation • Allergen-specific serum IgE • Still often referred to as RAST testing which is a specific lab test but RAST testing is outdated. The test is now CAP FEIA even when a RAST panel is ordered. • Not diagnostic when used alone to determine food allergy. • May be more accurate than SPTs to predict clinical reactions; the higher the level, the more likely a reaction will occur. • Does not always correlate with SPT • sIgEmeasures IgE in the serum • SPTs measure IgE bound to cutaneous mast cells
Allergen-specific serum IgE levels (Guidelines only) *Under age 2: Egg: 95% reaction risk for level of 2 kIU/L or more Milk: 95% reaction risk for level of 5 kIU/L or more
Food Allergy Evaluation • Elimination Diets • Especially useful for food allergies related to EoE • Eliminate a single food for 1-6 weeks or go to an elemental diet and slowly add food back in • Oral food challenges • Reasons to challenge • Confirm the diagnosis of food allergy • Determine whether a food allergy has been outgrown • Double blind placebo controlled food challenge- gold standard but not usually done for diagnosis due to time and cost constraints • Open or single-blinded oral food challenges acceptable- often done to see if patient is no longer food allergic (skin & blood tests are negative or significantly decreased) • Baked food challenge first
Food Allergy Diagnosis • Diagnosis is based on the results of SPT, serum IgEtesting, clinical history, and oral food challange. No single test or history alone can determine an IgE-mediated food allergy. • Oral Allergy Syndrome: Form of localized IgE-mediated contact allergy, usually to raw fruits or vegetables, with symptoms confined to lips, mouth, and throat. Most commonly affects patients who are allergic to pollens. Reactions are usually mild, anaphylaxis is rare. • Birch: apple, apricot, carrot, cherry, kiwi, plum • Ragweed: banana, cucumber, melon, watermelon • Grass: cherry, peach, potato, tomato
Seasonal and Perennial Allergy Testing • Seasonal • Trees, grass, weeds • Perennial • Dust mites, mold, animals • Causes an IgE-mediated reaction but anaphylaxis is not common • Reasons for testing • Patient wants to know • Help with pollen/animal avoidance • Immunotherapy • Help control co-morbid conditions (asthma, atopic dermatitis) • Improve quality of life
Bee Venom & Antiobiotic Testing • Bee venom testing • Testing is not done if only reaction is a large local • Types of vespids tested • Honey bee • Yellow Jacket • White-faced hornet • Yellow hornet • Wasp • Antibiotic testing • Pen VK is the only antibiotic with standardized testing but all antibiotics can be evaluated • Testing done only for IgE-mediated reactions, not serum sickness or other types of reactions
Nonstandard and unproven procedures • TotoalIgG or Allergen-specific IgG4 • Applied kinesiology • Provocation neutralization • Hair analysis • Electrodermal testing • Basophil histamine release/activation • Lymphocyte stimulation • Facial thermography • Gastric juice analysis • Endoscopic allergen provocation • Cytotoxicity assays • Mediator release assay (LEAP diet)
Resources • Guidelines for the Diagnosis and Management of Food Allergy in the United States: Report of the NIAID-Sponsored Expert Panel, The Journal of Allergy and Clinical Immunology, Volume 12, Number 6, December 2010. • Food Allergy and Anaphylaxis Network, www.foodallergy.org • Utah Food Allergy Network, www.utahfoodallergy.org • American Academy of Allergy Asthma & Immunology, www.aaaai.org • American College of Allergy Asthma & Immunology, www.acaai.org