Download

1 / 18
190 likes | 338 Views
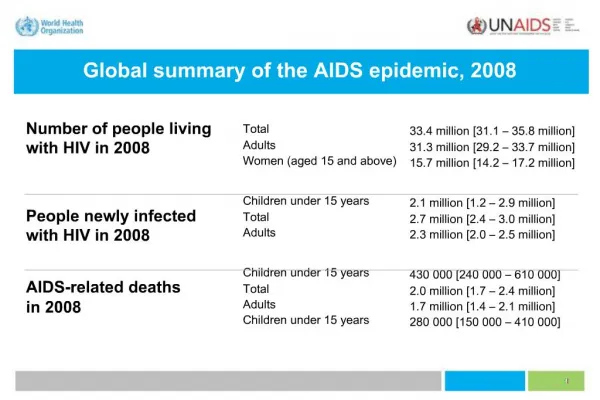
Sepsis Protocol Go Live December 1, 2009. Hendricks Regional Health. Phases of Sepsis. Phase I: SIRS (System Inflammatory Response Syndrome) Criteria Phase II: Septic Phase III: Severe Septic Phase IV: Septic Shock. SIRS – Phase I.

E N D
Sepsis ProtocolGo Live December 1, 2009 Hendricks Regional Health
Phases of Sepsis • Phase I: SIRS (System Inflammatory Response Syndrome) Criteria • Phase II: Septic • Phase III: Severe Septic • Phase IV: Septic Shock
SIRS – Phase I • SIRS (Systemic Inflammatory Response Syndrome) Criteria • Temp >38 C (100.4 F) or < 36 C (96.8 F) • HR > 90 • RR > 20 or PaCO2 < 32 or mechanical ventilation • WBC > 12,000 or < 4,000 or > 10% band forms
Sepsis – Phase II • The patient has Sepsis, if • 2 of 4 SIRS criteria present • suspected or confirmed source of infection
Severe Sepsis – Phase III • A patient withsepsis complicated by: • Tissue hypoperfusion (need fluid) • Elevated venous lactate (> 2.1 mmol/L) • Oliguria • Sepsis-induced hypotension • SBP < 90 • MAP < 65 mm Hg • Decrease in SBP of > 40 mm Hg below normal • Organ dysfunction
Septic Shock – Phase IV • Despite adequate fluid therapy, SBP < 90 or MAP < 65 • Sometimes difficult to distinguish between severe sepsis from septic shock • Carries a mortality rate of 40-60%
HRH Data Audited 44 patient charts in 2008: • Admitted with Sepsis diagnosis - 18 patients (41%) • Admitted to Med/Surg - 28 patients (63.6%) • FASTeam to ICU - 7 patients (25%) • Admitted to ICU - 16 patients (36.3%) • Met SIRS Criteria/Septic, different diagnosis than sepsis– 14 patients (31%)
Average cost of hospitalization $29,000 • Average hospital length of stay 7.3 days • Average hospital length of stay in ICU – 9.4 days • Death 2 patients (4.17%) • Xigris was not administered in 2008
Lactate Levels • Indication for tissue hypoperfusion and oxygenation • Elevated Lactates • > 2.1 mmol/L • Identified before the patient is hypotensive (early indication) • Common with severe septic and septic shock patients • All patients are to be started on the protocol, regardless of BP • Serial lactate levels are helpful to assess adequacy of therapies in shock patients • Lactate levels will be drawn q 3 hours x 3
Room for Improvement • Recognize early signs of Sepsis (41%) • Obtain venous lactate (0%) • Earlier initiation of pressors • Blood cultures obtained
Sepsis Resuscitation Bundle – First 6 hours • Measure venous lactate (other labs and tests: ABG, CBC, BMP, CK/Trop, urine cultures, sputum cultures, CXR) • Blood cultures obtained prior to antibiotic administration • Administer broad-spectrum antibiotics within 3 hours of ED admission and within one hour of non-ED admission • Hypotensive/serum lactate >2.1 mmol/L • Deliver 20 ml/kg of NS (adequate amount) • Administer Vasopresors for hypotension not responding to fluid resuscitation to maintain MAP > 65
Sepsis Resuscitation Bundle – ED/ICU • If hypotension continues after adequate fluid bolus and/or lactate level > 2.1 mmol/L, insert PreSep Catheter: • Central venous pressure (CVP) 8-12 mm Hg • Central venous saturation (ScvO2) >/= 70% • Temp-Sensing Foley Catheter: • Urine Output > 0.5ml/kg/hour • Temperature monitoring • Mechanical Ventilation • PaO2/FiO2 ratio </= 250 • Plateau Pressures < 30 • Start Vasopressors (norepinephrine preferred-need central line) • Xigris may be considered • If no central line, start dopamine and titrate to MAP >/= 65 or SBP >/= 90 mm Hg
Sepsis Management Bundle –(24 Hours) • Followed on any Severe Septic patient • Low dose steroids • Maintain glucose control greater then the lower limit of normal, but less then 150 mg/dl • GI Bleeding Prophylaxis • DVT Prophylaxis • Venous Lactate levels q 3 hours x 3
Enteral nutrition is preferred over parenteral because it is associated with improved patient outcomes. • Suggest initiate enteral nutrition when: • Patient is malnourished • Patient not expected to resume po within 5 days • Patient is fluid resuscitated and hemodynamically stable • Enteral feeding route can be established • There is no bowel obstruction distal to the site of feeding Information provided by: Robin Matejcek, Registered Dietitian at HRH
OXEPA • Complete, balanced nutrition formula with eicosapentanoic acid, gamma-linolenic acid, and elevated levels of antioxidants to help modulate the inflammatory response. • Use in critically ill patients with sepsis, ALI or ARDS clinically shown to: • Reduce markers of pulmonary inflammation • Improve oxygenation • Decrease requirements for vent support • Decrease ICU stay • Decrease development of new organ failures • Reduce mortality Information provided by: Robin Matejcek, Registered Dietitian at HRH
Conclusions • New sepsis orders are intended to smooth processes of care. • Nursing and other ED and ICU staff have been educated on the early recognition and aggressive resuscitation of sepsis patients. • For comments, please provide feedback to Adam Andres, David Farman or John Sparzo