Download
1 / 27
761 likes | 3.17k Views
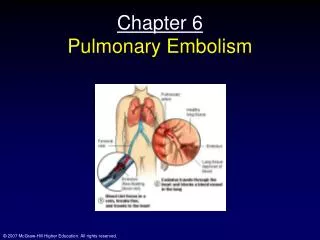
Chapter: 38 Pulmonary Circulation, Pulmonary Edema, Pleural Fluid. By Dr. Mudassar Ali Roomi (MBBS, M.Phil. ) Assist. Prof. Physiology. Physiological anatomy of pulmonary circulatory system. The pulmonary vessels the pulmonary arterial tree has a large compliance

E N D
Chapter: 38Pulmonary Circulation,Pulmonary Edema, Pleural Fluid By Dr. Mudassar Ali Roomi (MBBS, M.Phil.) Assist. Prof. Physiology
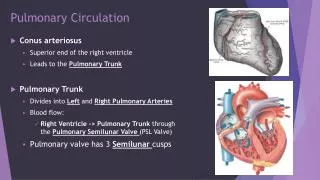
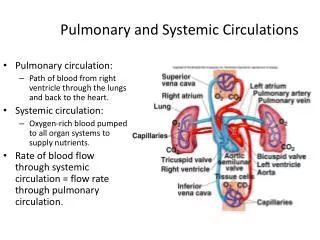
Physiological anatomy of pulmonary circulatory system • The pulmonary vessels • the pulmonary arterial tree has a large compliance • Bronchial blood vessels • 1 to 2 % of the total cardiac output. • the left ventricular output is about 1 to 2 % greater than the right ventricular output. • Lymphatic from the lungs enter into right thoracic lymph duct
Blood volume of the lungs • 500 milliliters • 9 % of the total blood volume of the entire circulatory system. • Approximately 70 ml in the pulmonary capillaries • Lungs as a Blood Reservoir (100-250 ml)
Automatic Control of Pulmonary Blood Flow Distribution • Hypoxia vasoconstriction • When concentration of oxygen in the air of the alveoli decreases below 70 % of normal ,the adjacent blood vessels constrict. • This is opposite to effect observed in systemic vessels • Undiscovered vasoconstrictor substance to be released from the lung tissue • Important function: to distribute blood flow to most oxygenated alveoli.
Pressure Pulse Curve in the Right Ventricle. • Systolic: 25 mm Hg • Diastolic: about 0 to 1 mm Hg
Pressures in the Pulmonary Artery. • Systolic: 25 mm Hg • Diastolic: 8 mm Hg. • Pulse pressure: 17 mm Hg.
Pulmonary Capillary Pressure: 7 mmHg • Left Atrial and Pulmonary Venous Pressures: • The mean pressure in the left atrium and the major pulmonary veins averages about 2 mm Hg • estimated with moderate accuracy by measuring the pulmonary wedge pressure (5 mm Hg). It is 2 to 3 mm Hg greater than the left atrial pressure
Comparison of pressures in systemic and pulmonary circulations.
Length of Time Blood Stays in the Pulmonary Capillaries (0.3-0.8 sec).
Effect of Increased Cardiac Output on Pulmonary Blood Flow and Pulmonary Arterial Pressure During Heavy Exercise • During heavy exercise, blood flow through the lungs increases fourfold to sevenfold. • This extra flow is accommodated in the lungs in three ways: (1) by increasing the number of open capillaries, (2) by distending all the capillaries (3) by increasing the pulmonary arterial pressure.
Shift of Blood Between the Pulmonary and Systemic Circulatory Systems as a Result of Cardiac Pathology (left heart failure). • affects the pulmonary system greatly but usually has only mild systemic circulatory effects.
Effect of Hydrostatic Pressure Gradients in the Lungs on Regional Pulmonary Blood Flow • Hydrostatic pressure is affected by gravity • Pulmonary arterial pressure at the apex of lung of a standing person is about 15 mm Hg less than the pulmonary arterial pressure at the level of the heart • The pressure in the base of the lungs is about 8 mm Hg greater than the pulmonary arterial pressure at the level of the heart.
Zones of Pulmonary Blood Flow Zone 1 blood flow • No blood flow during all portions of the cardiac cycle • Zone 1 Blood Flow Occurs Only Under Abnormal Conditions. • occurs when either the pulmonary systolic arterial pressure is too low or the alveolar pressure is too high to allow flow • Too high alveolar pressure e.g. Breathing against a positive air pressure • After severe blood loss.
Zones of PulmonaryBlood Flow • Zone 2 (intermittent fblood low) in the apices. • In normal lungs, this zone is about 10 centimeters above the midlevel of the heart and extends from there to the top of the lungs • Blood flows during systole but not during diastole. • Zone 3 (continuous blood flow throughout the cardiac cycle) in all the lower areas. • from about 10 centimeters above the level of the heart all the way to the bottom of the lungs,
Capillary Exchange of Fluid in the Lungs, and Pulmonary Interstitial Fluid Dynamics
STARLING FORCES: Capillary Exchange of Fluid in the Lungs, and Pulmonary Interstitial Fluid Dynamics
Negative Pulmonary Interstitial Pressure and the Mechanism for Keeping the Alveoli “Dry.”
Pulmonary Edema CAUSES • Left-sided heart failure • mitral valve disease • Damage to the pulmonary blood capillary membranes • Infections (pneumonia) • Breathing noxious substances such as chlorine gas or sulfur dioxide gas
Pulmonary Edema Safety Factor • pulmonary capillary pressure must rise from the normal level of 7 mm Hg to more than 28 mm Hg • Safety factor against pulmonary edema of 21 mm Hg.
Safety Factor in Chronic Conditions (>2 weeks) e.g. Chronic mitral stenosis • No lethal edema in chronic lung conditions. This is because Lymph vessels expand greatly and increase the drainage of fluid (upto 10 fold). • Pulmonary capillary pressures may rise upto40 to 45 mm Hg even without development of pulmonary edema.
Rapidity of Death in Acute Pulmonary Edema • A medical emergency • Cause: Acute left-sided heart failure • Pulmonary capillary pressure may rise more than 50 mmHg • Death frequently ensues in less than 30 minutes in severe cases
Pleural Cavity • the pleural space—the space between the parietal and visceral pleurae • It is a potential spaceonly • It contains only a few ml fluid. • a thin layer of mucoid fluid lies between the parietal and visceral pleurae for easy slippage of moving lungs.
The pleural membrane • serous membrane through which small amounts of interstitial fluid transude continually into the pleural space. • Pumping of fluid from the space by the lymphatics provides negative pressure in pleural cavity (–7 mm Hg).
Pleural Effusion • Definition: Pleural effusion means the collection of large amounts of free fluid in the pleural space. • The effusion is analogous to edema fluid in the tissues and can be called “edema of the pleural cavity.” Causes: • Blockage of lymphatic • Cardiac failure • Greatly reduced plasma colloid osmotic pressure • Infection or any other cause of inflammation