Download
1 / 23
250 likes | 611 Views
St. Martin de Porres Charity Hospital Emergency Department. Operations Management Final Paper ANGUSTIA, BERNADETTE C. VEGA, ALFONSO GABRIEL A. St.Martin de Porres Charity Hospital. 1959 – Blessed Martin de Porres Medical Free clinic Handled by Dominican Priory

E N D
St. Martin de Porres Charity Hospital Emergency Department Operations Management Final Paper ANGUSTIA, BERNADETTE C. VEGA, ALFONSO GABRIEL A.
St.Martin de Porres Charity Hospital • 1959 – Blessed Martin de Porres Medical Free clinic • Handled by Dominican Priory • 1965 – Medicine, Pediatrics, Dental, Nutrition, Laboratory • Later on became an infirmary “St. Martin de Porrese Charity Hospital” • 1979 – classified as 30-bed secondary hospital • 1983 – classified as a TERTIARY Hospital
St.Martin de Porres Charity Hospital • Currently a 150-bed capacity tertiary hospital • Services offered: • Surgery – main service • Medicine • Pediatrics • Obstetrics and Gynecology • Radiology • Nutrition • Dentistry • Ophthalmology • ENT • Emergency Medicine
SMPCH’s VMO • Vision: • aims to provide quality and affordable medical and healthcare services to the less privileged members of the society. • Mission: • Inspired by God’s love, the hospital fosters a work environment where volunteers, professionals and benefactors take active and compassionate interest in the patients they serve.
SPMCH’s VMO • Primary Objective: • Medical service for the indigent sick members of the society giving higher priority to the charity patients over paying patients (who may have better possibilities to secure personal medical services in other hospitals).
SMPCH ER • TRIAGE • Non-urgent • Urgent • Emergent • Stabilize patient • Referral to proper service
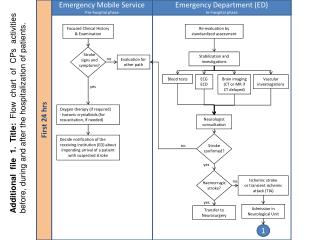
Patient arrives at ER Triage Does the patient have an Ob-Gyne complaint? Patient is decked under Ob-Gyne service. Y N Is the patient<18?years old Y Patient is decked under pediatric service. N Will the patient need surgery? Patient is decked under Surgery service. Y N Patient is decked under Internal Medicine service. Patient is examined by the physician on duty. Patient is given appropriate treatment. Process Flowchart
Patient is reassessed. Will the patient be admitted? Patient pays ER bill at window 1 Patient returns official receipt to ER NOD. Companion is given OPD record and brought to admission. Patient is given home instructions and OPD follow-up . Data sheet is brought to the ER by admitting staff. Ward is informed by the ER NOD and admitting section Patient is sent home. Patient is brought up to the ward. Process Flowchart
Patient Arrival Data: Descriptive Analysis • Direct observation of patient arrivals • Average influx: 60 patients for 2 days • Ave. No. of patients: 30 per day • 47% involved abdominal pain and fever
Patient Arrival Data: Descriptive Analysis • Patient arrival: • 6am-2pm shift- 20 patients (33.33%) • 2pm-10pm shift – 28 patients (46.67%) • 10pm-6am shift – 11 patients (18.33%) • Average time to evaluation from time the patient comes in is 35 MINUTES. • Longest time to be seen recorded 5 hrs 20 mins • Shortest time recorded is under a minute
Patient Arrival Data: Descriptive Analysis • Longest discharge time – 10 hrs 32 mins • Fastest discharge time – 5 mins • Primary Services: • Medicine 20 patients (33.33%) • Pediatrics 18 patients (30%) • Surgery 11 patients (18.33%) • Obstetrics 10 patients (16.67%)
Poka-Yoke System • Referral Logbook • Keep track of referrals • Monitor time response • Quality control tracker of services • Out-source diagnostics and imaging modalities • Business agreement with diagnostic centers • MOA prioritizing SMPCH patients • Lab result delivery
Poka-Yoke System • User-friendly ER forms and Pathway forms • Lessen writing/charting time • Symptom-specific pathway forms help facilitate faster more efficient flow • Help lessen human error
Conclusion • OpMan tools helped identify relevant and quantifiable observations • Main causes of lag in patient care in the ER: • Long physician waiting time • Unavailability of medications and supply • Delay in imaging and laboratory exams
Conclusion • Recommendations • Service referral log books • Symptom-specific pathway forms • Outsource laboratories and imaging exams • Scope and Limitation • Main focus: FEASIBLE ACTIONS given the circumstance that would be easily implemented • Recommendations involving increase in capital investments were not inquired into as much