Download
1 / 57
570 likes | 584 Views
Learn about the general functions of the circulatory system, including oxygen transport, nutrient distribution, waste removal, temperature regulation, and more. Discover the major components of the human circulatory system, such as blood vessels and the heart, and understand the role of arteries, arterioles, and capillaries in blood circulation.

E N D
General Functions of the Circulatory System • a. To transport inhaled oxygen from the lungs to the cells of the body for cellular respiration. b. To transport CO2 from the cells of the body to the lungs for exhalation. • To distribute nutrients from the villi capillaries to all cells of the body. • To transport: a. Metabolic (nitrogenous) wastes to the kidneys, including urea. b. Toxic substances to the liver.
To distribute hormones to the tissues/organs on which they act. • To regulate body temperature: i. Donation/absorption of heat ii. Flow shunting • To prevent blood loss through blood clotting. • To protect the body from pathogens (viruses/bacteria) due to the circulation of antibodies and white blood cells.
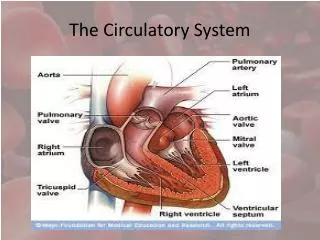
DEFINITIONS: (see fig. 13.7 p. 246) Systemic Circulation – Blood pumped by the LEFT side of the heart, which services the entire bodyexcept the lungs. Pulmonary Circulation – Blood pumped by the RIGHT side of the heart, which services only the lungs. ‘Services’ = provides O2 & nutrients, while carrying away CO2 and other wastes.
The Major Components of the Human Circulatory System • Blood Vessels (5 types) • Blood • Heart
Blood Vessels (refer to fig. 13.1 p. 240) • Arteries • Carry blood AWAY from the heart. • Arteries possess the thickest walls of all vessel-types. • Their walls possess three layers of tissue: i. Inner epithelial layer (aka endothelium)- possesses elastic fibers and is very smooth to promote easy flow. ii. Middle smooth muscle layer (contracts or relaxes to regulate blood flow and pressure) * the thickest layer iii. Outer fibrous epithelial tissue which serves a protective function. It is comprised of elastic fibers allowing stretching and recoiling. Note: Veins also possess three layers of tissue, but their walls are not as thick as those of arteries.
Vein Artery • The walls some major arteries (eg. Aorta) are so thick, they must be supplied by their own blood vessels. • Arteries in the systemic circuit carry oxygenated blood, whereas arteries in the pulmonary circuit carry deoxygenated blood. • Notice the smaller inner diameter of arteries compared to that of veins – this, due to the thicker middle muscle layer in arteries.
ii. Arterioles • Arterioles are vessels into which arteries have been divided. Arterioles have the same structure as arteries, but are simply smaller (they are barely visible to naked eye). • It is easier for blood to enter arteries (from the heart or other arteries) than it is for blood to exit arteries and enter arterioles (due to the smaller diameter of arterioles) this creates noticeable/measureable blood pressure during both heart contraction (systole) AND relaxation (diastole). • Pressure is measureable during diastole because arteries are never fully emptied of blood. • This impedance by the arterioles is known as peripheral resistance. • When we measure our pulse, we count the elastic expansion of artery walls upon systole. When we measure our blood pressure, devices are able to deduce the pressure in arteries during systole AND diastole (due to peripheral resistance). • The perpetual pressure within arteries, due to peripheral resistance, keeps blood flowing even when the heart is relaxing (diastole).
Flow Shunting • Blood flow into arterioles, and eventually capillaries, is controlled in two ways (governed by nerve and/or endocrine signals) (see fig. 13.2 p. 241): • Smooth muscles lining arterioles constrict, thus allowing less blood to enter; however, the arteriole does not fully close, so some blood enters… • The ‘back-up’ plan involves pre-capillary sphincter muscles contracting or relaxing in order to respectively close or open access into capillary beds; if closed off, blood flows to venules through a thoroughfare channel so that it can reach more ‘useful’ areas more quickly.
Why restrict access to arterioles/capillaries (ie. Why Flow Shunt)??? • Example scenarios: • Cold weather; want blood (with heat) to flow to the core of the body, not periphery…blood gets shunted to core through the ‘closing off’ of the peripheral arterioles/sphincter muscles. • Exercising; want blood (with O2 and nutrients) to flow to skeletal muscles and heart, not the digestive tract or other non-necessary places…blood gets shunted to muscles. Good or bad to exercise after eating and why? • Relaxing; blood shunted to digestive tract to pick up nutrients etc…
iii. Capillaries • Capillaries are tiny vessels with walls that are one cell thick, thus allowing for the efficient exchange of substances. • They are evident in all bodily regions (very high cross-sectional area)…almost all cuts draw blood. • Their small diameter only allows ‘single file’ passage of red blood cells (again, helps with efficient exchange of, in this case, oxygen and CO2). • They surround cells/tissues like a ‘spider web’ or ‘basket’. • Capillaries are, at most, 0.2 μm away from any cell in the body (further aids the exchange of substances). • Certain capillary beds may be open or closed depending on demands & subsequent flow shunting.
In general, only about 5-10% of the body’s blood is in the capillaries at any one time.
iv. Venules • Same structure as a vein (see below), only smaller. • Collect blood from the capillaries and/or the thoroughfare channels and join/enlarge to form veins. v. Veins • Thin-walled compared to arteries. -- this provides veins with a larger interior diameter than arteries. Thinner muscle layer
Same three layers of tissue as arteries, but the middle smooth muscle layer is thinner. • Carry blood TOWARDS the heart. • There exists a lower blood pressure in veins since they are further from the heart, and because of the larger interior diameter. • VALVES (one-way) assist with the upward (against gravity) movement of blood back to the heart (valves prevent the backflow of blood). Malfunctioning valve varicose vein. • Generally, 70% of the body’s blood is in the veins…act as somewhat of a blood resevoir.
ONE-WAY VALVES • Veins are located closer to the surface of the body than arteries, and they are surrounded by skeletal muscle. • The contraction of these skeletal muscles aid in blood flow through the veins (ie. The skeletal muscles are the “hearts” for the veins). • In the systemic circuit, veins carry deoxygenated blood. • In the pulmonary circuit, veins carry oxygenated blood
Blood Pressure and Blood Velocity (fig. 13.9 p.248) Blood Pressure (BP): The hydrostatic pressure that blood exerts against the wall of a vessel. • highest in arteries due to their receiving of blood from the heart and due to the peripheral resistance created by the smaller arterioles. • that said, the BP within arteries varies with respect to the heart contracting (systole) and relaxing (diastole) systolic pressure is higher than diastolic pressure. • BP begins to drop in arterioles as the blood simply gets further from the heart’s push, and it ‘spreads out’ more. • BP in the capillaries is somewhat ‘medium’ in that even though the blood is far from the heart’s pump, the vessel openings are small and the walls are thin allowing for a greater hydrostatic pressure against them.
By the time the blood reaches the veins, its pressure is not affected much by the heart due to its travel (and coupled ‘slow-down’) through tiny-diameter arterioles and capillaries. • Thus, very low BP in veins (the lowest, in fact): • Blood is furthest from heart; • Blood experienced extreme resistance within arterioles/capillaries; • Veins possess a very large (relative to arteries) interior diameter. *BP can also increase with higher blood volume!
Blood Velocity: the speed of blood moving through vessels. • blood velocity is highest in the arteries due to the heart’s pump; • Blood velocity is lowest in the capillaries due to the single-file RBC flow through them and the massive ‘spreading-out’ of the blood to the millions of capillary beds in the body; • Blood velocity picks up again (but not to the arterial level) in veins due to their large interior diameter (‘freeway’) and due to the action of skeletal muscles to propel the blood back to the heart. * The cross-sectional area (area of vessel wall in contact with blood) of the vessels is greatest in capillaries and lowest in arteries and veins.
Major Blood Vessels (fig. 13.8 p. 247) Red vessels: usually arteries except for pulmonary circuit. Carry oxygenated blood. Blue vessels: usually veins except for pulmonary circuit. Carry de-oxygenated blood.
Aorta – carries oxygenated blood out from the Left Ventricle of the heart and services the entire systemic circuit by eventually branching into various arteries. *Houses special nerves cells (Aortic Bodies) that sense H+, CO2, and O2 levels in blood. • Coronary Arteries and Veins – Arteries: branch off of the aorta and service the actual heart muscle (these vessels are seen on the surface of the heart) (*Blood in the heart’s chambers does not actually service the heart). Coronary Veins: carry ‘spent’ blood back to the heart’s chambers. • Carotid Arteries – branch off of the aorta to service the brain/head region. Highly specialized contain special nerve cells (Carotid Bodies):
i. Chemoreceptors that detect O2, H+, and CO2 content in the blood. ii. Pressure Receptors that detect blood pressure changes. -- the carotid artery can be used to measure one’s pulse. • Jugular Veins – opposite of carotid arteries. Carry blood from the brain/head region back to the heart. Possess no valves since gravity aids the flow. • Subclavian Arteries/Veins – service the arms. Within the right subclavian vein there is a union between the lymphatic system and the circulatory system.
Mesenteric Arteries – carry blood from the aorta to the intestines (gut). Subdivide into villi capillaries. • Hepatic Portal Vein – carries blood from the intestines to the liver. *Hepatic = liver-related • Hepatic Vein – carries blood from the liver back to the heart. • Renal Arteries/Veins – service the kidneys. *Renal= kidney-related 10. Iliac Arteries/Veins – service the legs.
Superior (Anterior) and Inferior (Posterior) Vena Cavae– collect/receive all of the blood from the various veins of the systemic circuit and conduct it back into the right atrium of the heart. Superior Vena Cava – collects blood from above the heart. Inferior Vena Cava – collects blood from below the heart. 12. Pulmonary Arteries/Veins – only major vessels of the pulmonary circuit. Pulmonary arteries carry deoxygenated blood from the heart to the lungs. Pulmonary veins carry oxygenated blood from the lungs back to the heart. * Pulmonary Trunk – first vessel to receive blood (bound for the lungs) from the heart. Splits into two pulmonary arteries (one for each lung).
Aorta The aorta and the coronary system…heart not shown.
Blood • Made up of, and will separate into, two components: • Plasma – comprises 55% of the blood volume • Formed Elements (Cells) – comprise 45% of the blood volume. - includes Red Blood Cells (RBCs), White Blood Cells (WBCs), and Platelets (which are simply cell fragments). *fig. 13.10 p. 249.
Plasma • 90-92% water maintains blood volume and pressure; transports substances due to its flowing and polar nature; regulates temperature. Primarily absorbed by small and large intestines. • 7-8% Plasma Proteins maintain blood O.P./volume, etc. Produced by the liver. Too large to leave blood through capillary exchange. • Albumins: maintain BP and blood volume; transport bilirubin. • Immunoglobulins: antibodies that fight infection (pathogens); transport cholesterol. • Fibrinogen/Prothrombin: aid in blood clotting.
<1% of the following combined: • Salts/Electrolytes (aka minerals): maintain OP and BP, pH, and aid in metabolism in many ways; absorbed primarily in small intestine. • Gases: oxygen/carbon dioxide from lungs/tissues respectively; • Nutrients: fats, glucose, amino acids from small intestine; • Nitrogenous wastes: urea, uric acid, ammonia, and creatinine from liver; • Hormones to aid metabolism; • Vitamins from small intestine to aid in enzymatic reactions (vitamins act as coenzymes).
Formed Elements Red Blood Cells (RBCs) – fig. 13.11 p. 250 • aka erythrocytes, RBCs are the most numerous of the blood cells; there exist about 25 trillion in our (on average) 5 L of blood (in fact, RBCs comprise 99% of blood cells). • Structure promotes Function: • RBC is a biconcave disk (flatter in center) allowing them to thread through capillaries very efficiently and providing them with a large SA to Volume ratio. • Lack nuclei and mitochondria to help limit size – without nuclei, RBCs live (on avg.) 120 days and are then destroyed (by phagocytic cells through phagocytosis) in the liver or spleen. Without mitochondria, RBCs metabolize anaerobically so that they do not use the very oxygen that they carry, in order to make their ATP energy.
Large SA-to-volume ratio promotes RBCs’ main function: to transport O2 in the blood. • RBCs also transport CO2 and H+ ions, but to a lesser extent than O2. • Each RBC houses about 250 million molecules of hemoglobin(Hb), an iron-containing protein responsible for carrying O2 (primarily). • Hb is bright red when it is carrying O2 and purple-red when it is not. • Hb is made up of four tertiary proteins (two alpha, two beta), four heme groups, and four Fe2+ ions. It can carry up to four O2 molecules at any one time. • When RBCs are destroyed/recycled, Hb’s iron is sent to the bone marrow to be reused; heme is converted into bilirubin in the liver (released as a part of bile); and the alpha and beta chains are hydrolyzed and the amino acids reused.
Hb picks up O2 (and drops off CO2) in the lung capillaries and transports it to other cells in the body, where it then gives up the O2 (and picks up CO2) so that it can diffuse into the respective cells. The diagram on the left provides information on how Hb ‘behaves’ differently in these different regions of the body.
Manufacture of RBCs (fig. 13.12 p. 251) - RBCs are primarily formed in the marrow of large bones: - bones of the chest (ribs/sternum), upper arms (humerus), upper legs (femur), lower arms (radius/ulna), lower legs (tibia/fibula), hips, skull. - multipotent stem cells in the bone marrow become erythroblasts (RBC precursor), which lose their nuclei, gain hemoglobin, and mature or differentiate into an erythrocyte (RBC). - Certain hormonal/nervous signals ‘tell’ stem cells how to develop as they have the ability to form any type of blood cell.
Control of RBC Production • Oxygen-sensitive chemoreceptors in various locations (medulla oblongata, aortic/carotid bodies, renal artery, hepatic vein) sense low O2 levels in the blood. • Stimulus sent to kidney to produce the hormone erythropoietin (EPO), which stimulates production of RBCs in bone marrow, and acts to slow the rate of RBC destruction – this allows for more O2 to be carried in the blood as we exhale plenty of it. • Once O2 levels are restored, chemoreceptors send negative feedback message to kidney to cease release of erythropoietin. • Some causes of lower than average O2 levels: exercise, loss of blood, high altitudes, poor hemoglobin/RBC production/formation (anemia) • Most common cause of anemia is iron deficiency.
Blood Typing A couple of definitions: Antigen – a substance that elicits a defensive response from the immune system. In the case of RBCs, an antigen (if present) is a protein that is displayed on the surface of the cell and serves as an ID tag for that cell. Antibody – an antigen-binding protein, produced by certain WBCs, that bind to certain antigens, ‘tagging’ them for destruction by phagocytic WBCs. FYI: Anti-gen = Antibody generating
See table 14.2 p. 278 for Pop’n distribution O most common, then A, then B, then AB… ABO System Key Points: If antibody B (say) comes into contact with antigen B, it will tag each B antigen for destruction (the blood clumps and causes flow problems). Antibodies exist only in the plasma. Donated blood is made up of primarily RBCs only. So…a person with AB blood can receive blood from anyone; whereas, a person with type O blood can donate to anyone. AB = Universal Recipient; O = Universal Donor.
Another Antigen: Rh protein (see fig. 14.13, p. 279 – excellent figure!) An Rh antigen is present in people with Rh+ blood (no antibody), and is not present in people with Rh- blood (also, no antibody). If a person who is Rh- is exposed to Rh+ blood, antibodies will then be produced that will tag each Rh+ RBC for destruction…happens often during a pregnancy where a mother is Rh- and her fetus is Rh+…the fetus’ RBCs move across the placenta (late in the pregnancy or during delivery, when the placenta begins to break down) and stimulate the mother to produce Rh antibodies which can then cross the placenta (usually in a subsequent pregnancy) to tag and destroy the fetus’ RBCs. Solved by injection of anti-Rh antibodies during, or just after, delivery of ‘first’ child, which destroy any Rh+ RBCs that entered the mother’s system, leading to prevention of production of Rh antibodies in mother and ‘saving’ second fetus if he/she is Rh+ as well.
White Blood Cells (WBCs) (fig. 13.10 p. 249) • aka Leukocytes • Can be granular or agranular. • Very large in size (have a nucleus) relative to RBCs and platelets. • In general, WBCs fight infection and resist disease by aiding in the development of immunity. • Produced in the bone marrow from the same stem cells as RBCs, but follow a different developmentalpathway. Two Classes and Five Types: Class I: Granular Leukocytes (filled with vesicles of enzymes that ‘defend’ against ‘invaders’) a. Basophils – release histamines that cause allergic reactions (clotting of area, dilation of vessels to allow neutrophils/monocytes to arrive).
b. Eosinophils – attack parasites by releasing substances that kill them. c. Neutrophils – attack and engulf foreign invaders, destroying themselves in the process (pus); aka phagocytes. Most numerous (60-70% of WBCs). Class II – Agranular Leukocytes • Monocytes (Macrophages) – like neutrophils except that they possess pseudopodia (‘arms’) that can extend out to capture invaders. As well, they may live through an encounter and even act to engulf dead neutrophils. • Lymphocytes (T and B) – produce antibodies that tag specific invaders for destruction.
Colony-stimulating Factors (CSFs) are secreted by ‘living’ WBCs to promote the WBC developmental pathway, leading to an increase in WBC production (akin to EPO for RBCs).
RBC = R Agranular WBC (Monocyte) = M Granular WBC (Eosinophil) = E M
Platelets (fig. 13.14 p. 254) – Cell Fragments • regulated by hormone thrombopoietin, which is released by the liver and/or kidneys when platelet counts are low. • They lack a nucleus; are fragments of megakaryocytes, which are derived from bone marrow stem cells. • Play a major role in blood clotting; when a blood vessel is broken, it must be repaired. In order for the tissue to regenerate, the blood flow through the cut must be stopped; a clot serves this function. • When a cut occurs, platelets congregate and stick to the irregular surface created by the cut. • If it is a minor cut, this congregation clogs the hole. • If it is a major cut, a sequence of events takes place: