Download

1 / 21
240 likes | 493 Views
Q fever. Overview. “Query” fever First described in Australia World wide zoonosis Caused by the bacterium Coxiella burnetii. Infectious Agent. Coxiella burnetii obligate intracellular organism organism very stable in environment resistant to drying, chemicals and may disinfectants.

E N D
Overview • “Query” fever • First described in Australia • World wide zoonosis • Caused by the bacterium Coxiella burnetii
Infectious Agent • Coxiella burnetii • obligate intracellular organism • organism very stable in environment • resistant to drying, chemicals and may disinfectants. • two antigenic phases: phase I and II • phase I (lipopolysaccharide present) - as found in nature, virulent • phase II (partial loss of lipopolysaccharide) - as found after multiple laboratory passages, less infectious
Epidemiology • Occurrence • worldwide, endemic in every part of the world except New Zealand. • esp. prevalent in meatworks, dairies and animal farms therefore making Q fever an occupational hazard • Reservoir • cattle, sheep, goats, some wild animals,ticks, domestic cats
Clinical Notes • Clinical signs often subclinical or extremely mild • Infection can be acute or chronic • Acute infection • no typical form of acute Q fever, although there are generally 3 major presentations 1) Self-limited flue-like syndrome 2) Pneumonia 3) Hepatitis
Clinical Notes cont... • Chronic Q fever • lasts more than 6 months • occurs in approx. 5% of patients infected with C. burnetii • C. burnetii multiplies in macrophages • heart is the most commonly involved organ • of all cases of endocarditis it represents:- • 3% in England and Lyon (France) • 15% in Marseille (France)
Clinical Notes cont... • Mode of Transmission • airborne dissemination of organisms in dust and direct contact with infected animals • transplacental transmission congenital infection. • blood transmissions • intradermal inoculation • ticks transmit to domestic animals but not to humans. • sexual transmission suspected. • Incubation Period • Usually 2-3 weeks • Treatment • Tetracycline and rifampin
Antibody response • Antibodies to phase 1 • indicates chronic infection • Antibodies to phase 2 • IgM & IgA appear shortly after onset of symptoms & may persist for up to 3 months • IgG appears shortly after IgM & remain for life • indicates acute infection but also persist throughout chronic infection. • phase 2 molecules are highly immunogenic compared to phase 1 • phase 1 molecules are masked in acute infection and therefore not exposed to the host’s immune system
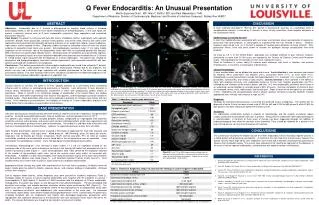
Diagnosis • Culture • Complement fixation test (CFT) • Indirect immunofluorescence assay (IFA) • ELISA
Culture • Hazardous • Not routinely used • Requires specially equipped laboratory
CFT • Usually phase II antigen • CF antibodies may not be detectable early in acute infection • CF antibodies may persist for months/years • Usually requires paired sera
IFA • Accepted method of diagnosis (“Gold Standard”) • More sensitive than CFT • Can measure individual antibody classes to different phase and can therefore be used to distinguish between acute & chronic infection • Ideal for confirmation and small volume testing
ELISA • More sensitive than IFA (IgG studies) • Very specific • Suitable for large scale screening • Diagnosis can be based on single serum specimen when IgM ELISA used • Can measure responses to different classes of antibody
Panbio Q fever ELISAs C. burnetii (Q fever) IgG ELISA Cat # E-QFB01G C. burnetii (Q fever) IgM ELISA Cat # E-QFB01M • Phase II antigen • Ideal for laboratory use • 1hr 10min assay time • IgG and IgM kits available • Proven performance 1,2,3 • IgM ELISA sensitivity 99%, specificity 88%1 • IgG ELISA sensitivity71%, specificity 96% 2; sensitivity 98.4%, specificity 95.7% (compared to IFA using cutoff titre of 1/160)3
Panbio Q fever Dip-S-Tick C. burnetii Total Ig Dip-S-Tick kit Cat# D-QFB03T • Has dots for both Phase I and Phase II antigens. • Three dots are for Phase II (acute infection) determination and one is for Phase I (chronic infection) determination. • Built in control well indicates test has worked correctly • Convenient for small-volume testing • No special equipment other than a 50°C waterbath required • Semi-quantitative
Panbio Q fever IFA C. burnetii (Q fever) IFA Slides Cat#I-QFB01X • Contain both Phase I and Phase II purified organisms as well as a normal yolk sac (NYS) control. • All three are represented on each well of the slides as distinct microdots (figure 1). • Dilutions of the patient's serum are placed in wells on the slide, permitting the antibody to bind specifically to the organisms. Bound antibodies are tagged with a fluorescein labeled anti-human conjugate and observed using a fluorescence microscope. In this format, organisms are readily identified as small coccobacilli. Fluorescent coxiellae are bright yellow against a dull red background (counterstain).
Panbio Q fever IFA Figure 1 Dot configuration in slide well as seen through the microscope
Promotional Resources • Clinical Sheet • Publications • General • Panbio Q fever ELISAs • Newsletter articles
References • Field P. et al. (2000) J. Clin. Microbiol. 34(4):1645-47. • Field P. et al (2002) J. Clin. Microbiol. 40(9):3526-29. • D’Harcourt et al. (1996) Eur. J. Clin. Micro. Infect. Dis. 15:749-52.