Download
1 / 1
10 likes | 118 Views
Assessment of incidence, severity and treatment of pruritus caused by neuraxial opioids in obstetric population P.K.B.C. Raju, P.Johnston Department of Anaesthesia, Ninewells Hospital and Medical School, Dundee DD1 9SY. Assessment of Pruritus - Spinal. 60. 55. 55. Incidence of pruritus.

E N D
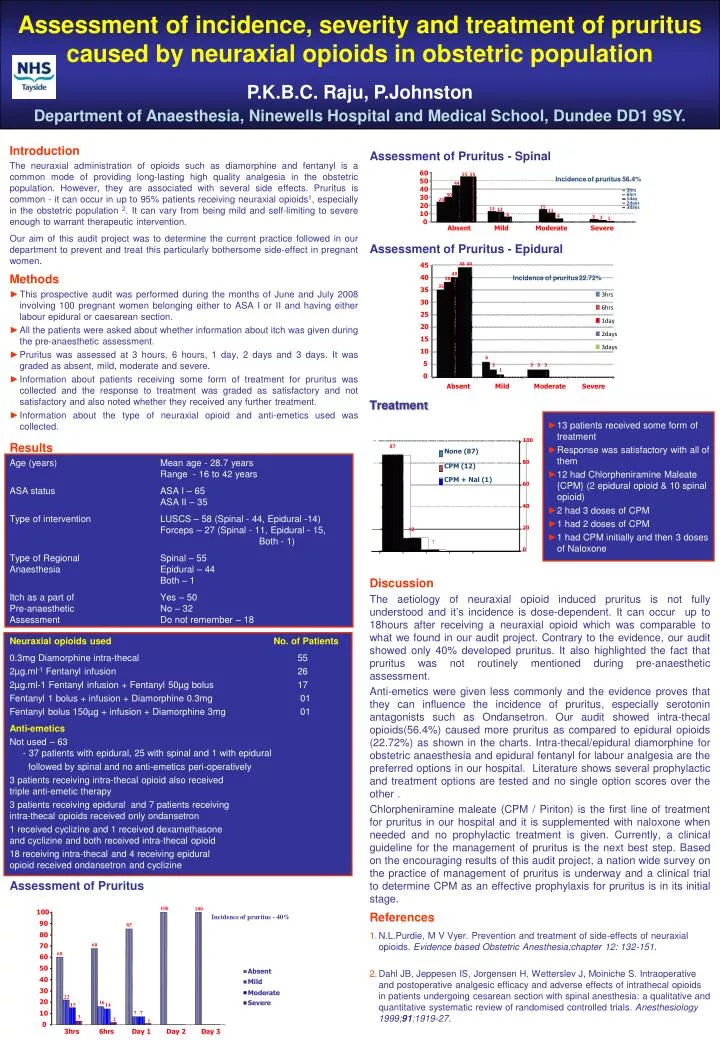
Assessment of incidence, severity and treatment of pruritus caused by neuraxial opioids in obstetric populationP.K.B.C. Raju, P.JohnstonDepartment of Anaesthesia, Ninewells Hospital and Medical School, Dundee DD1 9SY. Assessment of Pruritus - Spinal 60 55 55 Incidence of pruritus 56.4% 50 44 40 3hrs 6hrs 30 30 1day 24 2days 20 15 3days 13 12 11 10 6 4 3 2 1 0 Absent Mild Moderate Severe 100 87 None (87) 80 CPM (12) 44 44 45 CPM + Nal (1) 60 40 40 Incidence of pruritus - 22.72% 38 40 35 35 3hrs 20 12 30 1 6hrs 0 25 1day 20 2days 15 3days 10 6 5 3 3 3 3 1 0 Absent Mild Moderate Severe Assessment of Pruritus 100 100 100 Incidence of pruritus - 40% 90 85 80 70 68 60 60 50 Absent 40 Mild 30 Moderate 22 20 Severe 16 15 14 10 7 7 3 2 1 0 3hrs 6hrs Day 1 Day 2 Day 3 Introduction The neuraxial administration of opioids such as diamorphine and fentanyl is a common mode of providing long-lasting high quality analgesia in the obstetric population. However, they are associated with several side effects. Pruritus is common - it can occur in up to 95% patients receiving neuraxial opioids1, especially in the obstetric population 2. It can vary from being mild and self-limiting to severe enough to warrant therapeutic intervention. Our aim of this audit project was to determine the current practice followed in our department to prevent and treat this particularly bothersome side-effect in pregnant women. Assessment of Pruritus - Epidural • Methods • This prospective audit was performed during the months of June and July 2008 involving 100 pregnant women belonging either to ASA I or II and having either labour epidural or caesarean section. • All the patients were asked about whether information about itch was given during the pre-anaesthetic assessment. • Pruritus was assessed at 3 hours, 6 hours, 1 day, 2 days and 3 days. It was graded as absent, mild, moderate and severe. • Information about patients receiving some form of treatment for pruritus was collected and the response to treatment was graded as satisfactory and not satisfactory and also noted whether they received any further treatment. • Information about the type of neuraxial opioid and anti-emetics used was collected. Treatment • 13 patients received some form of treatment • Response was satisfactory with all of them • 12 had Chlorpheniramine Maleate {CPM} (2 epidural opioid & 10 spinal opioid) • 2 had 3 doses of CPM • 1 had 2 doses of CPM • 1 had CPM initially and then 3 doses of Naloxone Results Age (years) Mean age - 28.7 years Range - 16 to 42 years ASA status ASA I – 65 ASA II – 35 Type of intervention LUSCS – 58 (Spinal - 44, Epidural -14) Forceps – 27 (Spinal - 11, Epidural - 15, Both - 1) Type of Regional Spinal – 55 Anaesthesia Epidural – 44 Both – 1 Itch as a part of Yes – 50 Pre-anaesthetic No – 32 Assessment Do not remember – 18 Discussion The aetiology of neuraxial opioid induced pruritus is not fully understood and it’s incidence is dose-dependent. It can occur up to 18hours after receiving a neuraxial opioid which was comparable to what we found in our audit project. Contrary to the evidence, our audit showed only 40% developed pruritus. It also highlighted the fact that pruritus was not routinely mentioned during pre-anaesthetic assessment. Anti-emetics were given less commonly and the evidence proves that they can influence the incidence of pruritus, especially serotonin antagonists such as Ondansetron. Our audit showed intra-thecal opioids(56.4%) caused more pruritus as compared to epidural opioids (22.72%) as shown in the charts. Intra-thecal/epidural diamorphine for obstetric anaesthesia and epidural fentanyl for labour analgesia are the preferred options in our hospital. Literature shows several prophylactic and treatment options are tested and no single option scores over the other . Chlorpheniramine maleate (CPM / Piriton) is the first line of treatment for pruritus in our hospital and it is supplemented with naloxone when needed and no prophylactic treatment is given. Currently, a clinical guideline for the management of pruritus is the next best step. Based on the encouraging results of this audit project, a nation wide survey on the practice of management of pruritus is underway and a clinical trial to determine CPM as an effective prophylaxis for pruritus is in its initial stage. Neuraxial opioids used No. of Patients 0.3mg Diamorphine intra-thecal 55 2µg.ml-1 Fentanyl infusion 26 2µg.ml-1 Fentanyl infusion + Fentanyl 50µg bolus 17 Fentanyl 1 bolus + infusion + Diamorphine 0.3mg 01 Fentanyl bolus 150µg + infusion + Diamorphine 3mg 01 Anti-emetics Not used – 63 - 37 patients with epidural, 25 with spinal and 1 with epidural followed by spinal and no anti-emetics peri-operatively 3 patients receiving intra-thecal opioid also received triple anti-emetic therapy 3 patients receiving epidural and 7 patients receiving intra-thecal opioids received only ondansetron 1 received cyclizine and 1 received dexamethasone and cyclizine and both received intra-thecal opioid 18 receiving intra-thecal and 4 receiving epidural opioid received ondansetron and cyclizine References • N.L.Purdie, M V Vyer. Prevention and treatment of side-effects of neuraxial opioids. Evidence based Obstetric Anesthesia;chapter 12: 132-151. • Dahl JB, Jeppesen IS, Jorgensen H, Wetterslev J, Moiniche S. Intraoperative and postoperative analgesic efficacy and adverse effects of intrathecal opioids in patients undergoing cesarean section with spinal anesthesia: a qualitative and quantitative systematic review of randomised controlled trials. Anesthesiology 1999;91:1919-27.






