Download

1 / 27
270 likes | 284 Views
Explore the impact of gender inequality on the national AIDS response, focusing on women, girls, men who have sex with men, and transgender persons. Learn about relevant statistics, key actions, and recommended strategies for strengthening gender dimensions in HIV programs.

E N D
Contents of presentation • Women, girls and gender inequality • Men who have sex with men and transgender persons • 5 key actions
Sisonke self-help group for HIV positive people. (AVERT, photo_no_1255.)
I. Women, girls and HIV • 1995 to 2001 saw disproportionate increase in incidence of HIV among women and girls • Since then, rates have stabilized in most parts of the world, although variation between and within countries can be significant • In Sub-Saharan Africa, about 61% of all adults with HIV are women • Burden of care falls most heavily on women and girls • In most of the world, majority of HIV infections continue to be amongst males, and most women are probably infected within long-term partnerships / marriage – pointing to the connections between reproductive health and HIV • HIV rates among men who have sex with men and transgender persons are disproportionately high and climbing
Gender inequality, age and HIV Gender-based violence can cause HIV infection; stigma and discrimination can result in violence girls’ first sexual experience is often forced girls orphans and those married early are at increased risk also puts men and boys at risk Poverty gravely affects women’s and men’s ability to deal with the impact of AIDS; the denial of property and inheritance rights to women exacerbates the impact of HIV burden of care falls on girls who may leave school Keeping girls, as well as boys, in safe schools enhances effectiveness of prevention programmes education helps empower girls and women in their relationships and in escaping poverty education should challenge negative gender norms
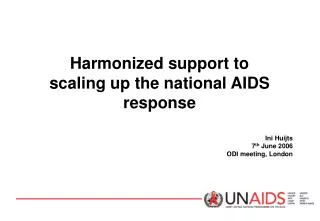
Percent of adults (15+) living with HIV who are female, 1990-2007 70 Sub-Saharan Africa 60 GLOBAL 50 Caribbean 40 Percent female (%) Asia 30 E Europe & C Asia 20 Latin America 10 0 1990 ‘91 ‘92 ‘93 ‘94 ‘95 ‘96 ‘97 ‘98 ‘99 ‘00 ‘01 ‘02 ‘03 ‘04 ‘05 ‘06 2007 Year Source: UNAIDS Report 2007
Methods for strengthening the gender dimensions of national AIDS responses: Objectives and Recommendations (1) 1. Know your country’s epidemic and current response in gender terms • Rec.1: Ensure that HIV monitoring, surveillance and evaluation fully capture information about the gender dimensions of the HIV epidemic, and periodically conduct stand-alone gender assessments to gather essential supplementary data. • Rec. 2:Assess the current AIDS response to see if and how it is addressing the gender dimensions of the epidemic
Objectives and Recommendations (2) 2. Plan, implement and evaluate specific actions to advance gender equality with appropriate attention across your multi-sectoral programme • Rec.3: Integrate gender into the national AIDS strategy, annual action plans and sector plans, with special attention being given to dedicated budgeting and allocation of funds. • Rec.4: Implement and scale up specific interventions to address the gender dynamics of the epidemic in your country in terms of HIV prevention, treatment, care and impact mitigation. • Rec.5: Develop and track targets and indicators to measure gender-related outcomes and impacts of AIDS programmes.
Objectives and Recommendations (3) 3. Build capacity and mutually reinforcing links between action on AIDS and broader action to achieve gender equality goals • Rec.6:Promote reciprocal capacity-building to increase the gender competence of those involved in AIDS-related initiatives and the HIV competence of those involved in gender-related initiatives. • Rec.7: Ensure the implementation of essential gender-related actions that promote the achievement of both AIDS-related goals and broader gender-equality goals.
Roles and responsibilities of key actors • National AIDS coordinating mechanisms • Civil society and grassroots organizations • Donors • UN agencies
a. National AIDS Coordinating mechanisms Provide vision; track infections; collect information; develop, fund and coordinate programming, engage all actors Ensure access to prevention, treatment, care, impact mitigation Assess legal and policy frameworks affecting females and males, with attention to people living with HIV, sexual minorities and marginalized populations Gather HIV/gender related information Engage civil society groups, gender-equality advocates, women living with HIV and human rights experts in assessment processes
b. Civil Society Actively engage as essential stakeholders Gather and disseminate crucial information Organize and advocate the active engagement of women living with HIV and those involved in gender-related activities in AIDS planning and funding processes Design innovative programming Develop strategies and capacity to monitor funding allocations and expenditure on gender-equality activities Expand participation and networks Facilitate partnerships and build synergies
c. Donor community Promote gender equality goals Provide sufficient funding for expansion of specific interventions to advance gender equality and address the needs of women and girls and integrate gender into other HIV-related activities Support efforts to connect sexual and reproductive health to HIV programming Assess own policies in terms of gender equality Coordinate actions to ensure that programmes that advance gender equality in national plans are fully costed Review funding to ensure gender equity Enhance harmonization
d. UN agencies Provide on-going and consistent support Offer technical support for the integration of gender into national AIDS strategy, as well as into sectoral plans and strategies Assess own policies to ensure gender integration Develop gender-focused activities and indicators and integrate gender equality as a cross-cutting priority in Joint UN Programmes Integrate gender into all global, regional and country-level guidance and programming tools developed to support the national AIDS response Earmark HIV resources for gender equality interventions
II. Sexual minorities • HIV rates among MSM are • extremely high in many regions: Asia, Caribbean, Latin America; • often rising again in high income countries; and • present but overlooked in Africa and Eastern Europe. • Most MSM infections around the world are occurring in “hidden” contexts of stigma and discrimination, criminalisation, rights abrogation and limited HIV surveillance • Only a small minority of countries report on coverage, and they report that only around 40% of MSM have access to the HIV prevention and care services they need • In all regions, transgender populations are among the most affected and most vulnerable
MSM and transgender populations • Unprotected anal sex (heterosexually, between men, or male/TG) particularly high risk behaviour • Anal sex together with sexual networking patterns means that male-male sex & TG sex contributes disproportionately to epidemic dynamics, compared to population prevalence of these behaviours / gender identities • Wide variation within and between societies on how male-male & TG sex is socially understood and constructed • Gender norms and notions of masculinity that exacerbate women’s vulnerability also impact MSM/TG populations
How many MSM have sex with men and with women? • How many MSM? • Few studies, but in East and South Africa, rates from 1-4% of pop is MSM (34% in South Asia • MSM and sex with women? • Caribbean –78% of MSM have ever had sex with women; 41% are married • Latin America –25% to 64% of MSM have ever had sex with women; 8% to 30% have had sex with women in the last year; data pooled from Central America shows 5% of MSM are married
Key actions on MSM/TG and HIV • Scaled up and more strategic country and community action, with leadership, commitment and follow up: • Know your epidemic in gender terms by including an MSM component in national sentinel surveillance; • Expand delivery of MSM-oriented public health services into community-based settings as appropriate; • Address violence perpetrated against MSM as it can exacerbate the HIV epidemic; • Strengthen technical capacity in design, execution and evaluation; • Support key actors at the national, local and community levels
Top five actions to improve national AIDS responses by addressing gender and AIDS (Office of the US Global AIDS Coordinator, AVERT photo_no_1459)
Actions (1) • Know your epidemic in gender terms • track and analyze HIV infection by sex, age, patterns of serodiscordance in couples, and how HIV differentially affects people by gender. • Involve all stakeholders in assessment, planning, governance, implementation and evaluation • women as well as men, positive women as well as positive men, young people, sexual minorities, sex workers, injecting drugs users, among others, all have different and crucial perspectives and knowledge to bring to the national AIDS response
Actions (2) • Identify and implement the right mix of actions • integrate a gender perspective into standard HIV interventions, and implement focused, stand-alone action on gender and AIDS. • Ensure that people and institutions focused on gender equality more broadly learn about HIV, and that people and institutions focused on HIV learn about gender equality. • Promote and act for gender equality and women's human rights more broadly
Assessing national AIDS response (1) • Overall, a limited consideration of issues around gender equality and sexuality • Impact of harmful gender norms on women AND men • Unequal power dynamics • Sexual violence and coercion • Limited knowledge of ‘how to’ apply gendered approaches • Include gender expertise and ‘hands on’ accompanied assistance. • Ensure assessment findings are pragmatic and strategic • Assessments need to be broadly consultative
Assessing national AIDS responses (2) • Insufficient efforts to identify, scale-up and mainstream promising practices • Identify positive projects that should be expanded. • These should help give guidance for a comprehensive, consistent approach • Lack of attention to structural issues that underlie gender inequality • It is important to look at how gender intersects with age, income, rural/urban location, and power dynamics to function as drivers of the epidemic