Download

1 / 31
310 likes | 467 Views
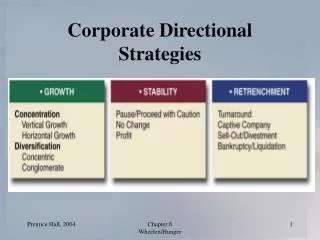
FUTURE STRATEGIES FOR MIDWIFERY IN TRINIDAD & TOBAGO. Betty Long, DNP, MPH, CNM, CNE, EFM-C, RNC-OB. MAIN FOCUS. ADMINISTRATION EDUCATION CLINICAL PRACTICE. GOAL. Nation’s Millennium Development Goal to reduce maternal deaths by 75% by 2015.6

E N D
FUTURE STRATEGIES FOR MIDWIFERYIN TRINIDAD & TOBAGO Betty Long, DNP, MPH, CNM, CNE, EFM-C, RNC-OB
MAIN FOCUS • ADMINISTRATION • EDUCATION • CLINICAL PRACTICE
GOAL • Nation’s Millennium Development Goal to reduce maternal deaths by 75% by 2015.6 • Maternal and infant mortality are indicative of the wellbeing of a nation • To improve practice by ensuring that all pregnant and recently delivered women receive the best possible care delivered in appropriate settings and taking account of their individual needs. • To reduce the maternal and infant morbidity and mortality ratio/rate: Main concern is with reproductive, maternal and child health
Environmental scan/SWOT Analysis • SWOT • Strengths • Weaknesses • Opportunities • Threats • Basic to any strategic or business plan development
Maternal Death • The death of a woman while pregnant or within 42 days of termination of pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes. (WHO)
Definitions of Maternal Death • Direct - Deaths resulting from obstetric complications of the pregnant state (pregnancy, labour and puerperium), from interventions, omissions, incorrect treatment or from a chain of events resulting from any of the above • Indirect - Deaths resulting from previous existing disease, or disease that developed during pregnancy and which was not due to direct obstetric causes, but which was aggravated by the physiologic effects of pregnancy
Definitions of Maternal Death • Late - Deaths occurring between 42 days and 1 year after abortion, miscarriage or delivery that are due to Direct or Indirect maternal causes • Coincidental (Fortuitous) - Deaths from unrelated causes which happen to occur in pregnancy or the puerperium • Pregnancy-related deaths - Deaths occurring in women while pregnant or within 42 days of termination of pregnancy, irrespective of the cause of the death
The Numbers • International: developed countries 1,600 women and over 5,000 newborn babies die daily due to complications that could have been prevented • MMR: 400 per 100,000 live births overall • UK 12 per 100,000 • US 7.1 per 100,000, NYS 20.5 hemorrhage – us 13.3 per 100.000 • Regional: Latin America/Caribbean 190 per 100,000 • National: T&T: 33.3 per 100,000
Beyond The Numbers • WH O, Beyond The Numbers: Reviewing Maternal Deaths and Disabilities to Make Pregnancy Safer • A detailed examination and evaluation of the problems in both determining a baseline MMR or interpreting what it actually means in helping to address the problems facing pregnant women in most developing countries.
Beyond the Numbers • Adopting this methodology to plan services will improve maternal and child health. • This concept of looking “beyond the numbers” to understand the real reasons why women die, through the use of a number of audit methodologies including confidential enquires, is now being promoted by the World Health Organization (WHO) as a key component of its Making Pregnancy Safer strategy.
ADMINISTRATIVE • Environmental scan or SWOT analysis • Midwifery education under the umbrella of SANE • To help inform government policy • To set minimum standards of care,
Administration • Promote annual mandates • Accurate recording of live births and stillbirths • Promote a Culture of Safety • Sentinel Event or Critical Incident Reporting • Use of vignettes to describe circumstances of maternal deaths and lessons learned
QUALITY ASSURANCE COMMITTEE • Monthly or quarterly • Review any near misses • Track and trend incidents • Root cause analysis of sentinel or critical events
EDUCATION • 5 yearly curriculum review to meet the needs of current patient acuity • Part of the postgraduate training and continuous professional self-development • Syllabus for all relevant health professionals to identify areas for further research
Simulation Use Validate skills Determine competency Evaluate team communication Prepare for life-threatening results Reduce error Improve safety
Shoulder Dystocia & Postpartum Hemorrhage Simulation Pictured above: L. Gioia, MD, A. Miller, RN, A. Hall, RN and other members of the L&D staff during a “Code Noelle” drill – Delivery complicated by Shoulder Dystocia and Postpartum Hemorrhage Courtesy Stonybrook University Hospital
Significance of Simulation • Students rarely allowed to participate when OB emergencies occur • More complex patients create the need for simulation • Experiential learning environment: • Safe • Risk-free • Non-threatening
CLINICAL PRACTICE • One methodology that has shown to be an effective communication method is SBAR • SBAR • S –SITUATION • B - BACKGROUND • A – ASSESSMENT • R - RECOMMENDATION
SBAR promotes: • Organization of information • Standardization of how we communicate • Across all disciplines caring for patient • Use of concise language • Avoiding unclear/ambiguous terms – “She’s doing fine”
S = SITUATION SITUATION describes: • What is going on with the patient • Concise statement of the problem • “I am calling you about Mary Doe. She is complaining of increased abdominal pain – right lower quadrant.”
B = BACKGROUND BACKGROUND describes: • What is the clinical background of the patient • Pertinent to the situation • “Mary Doe is post op day 2; status post open cholecystectomy”.
A = ASSESSMENT ASSESSMENT describes: • What is your assessment; what are your findings? • “She is alert; BP is elevated 130/96 from 110/80; Pulse = 120; Temp elevated to 1020 F; abdomen tender with guarding noted; Bowel sounds negative; urine output less than 20cc last 2 hrs; IV fluids – NS at 100cc/hr”
R = RECOMMENDATION Recommendation describes: • What action is needed to correct the problem • What do you want? • “Last labs were 6am; recommend repeat labs; I need you to assess patient. Would recommend holding pain meds till physical assessment done.”
Protocols/Policies/Guidelines • Implement, audit and regularly update local protocols for the referral of women with problems, or potential problems, in pregnancy and childbirth based on the health service delivery framework. • Local protocols should not only include the relevant clinical guidelines but also identify clear and agreed pathways of care and referral mechanisms for women who develop complications
Multidisciplinary Care • Coordinated multidisciplinary or multi-agency care should be available for all women with medical, mental health or social problems, including substance abuse and domestic violence, who may require specialist advice or support in pregnancy. • Women with complex pregnancies and who receive care from a number of specialists or agencies should receive the support and advocacy of a known midwife throughout their pregnancy
Annual Training • All medical and midwifery staff should be trained in: • Basic life support and neonatal resuscitation/HBB • Regular emergency drills for maternal resuscitation in all maternity units. • All health professionals: Regular and updated training on the impact of domestic violence, mental illness and substance misuse on the lives and health of pregnant women, their babies and families.
British Study • More than 50% of the women who died had some aspect of substandard clinical care. • Some died because their condition was not diagnosed or they received ineffective or the wrong treatment. • Not all care was consistent with current national clinical guidelines or provided by experienced staff.
Are Mothers Dying because? • They were unaware of the need for care, or unaware of the warning signs of problems in pregnancy? • The services did not exist, or were inaccessible for other reasons such as distance, cost or socio-cultural barriers? • The care they receive in traditional or modern health services is inadequate or actually harmful?
Further Research • To identify barriers which prevent women from seeking care or maintaining contact with the maternity services in order to help plan more appropriate service provision. • To estimate more robustly what, if any, is the degree of increased risk of maternal deaths associated with caesarean section particularly for those undertaken without a clinical indication. • To investigate the incidence of postpartum hemorrhage in relation to previous caesarean section and other direct causes
References Bambini, D., Washburn, J., & Perkins, R. (2009). Outcomes of clinical simulation for novice nursing students: Communication, confidence, clinical judgment. Nurse Educator’s Perspectives, 30(2), 79-82. Bantz, B., Dancer, M.M., Hodson-Carlton, K., & Van Hove, S. (2007). A daylong clinical laboratory: From gaming to high-fidelity simulation. Nurse Educator, 32(6), 274-277. Department of Health. Building a Safer NHS for Patients. London: Department of Health; 2001[www.doh.gov.uk/buildsafenhs]. Department of Health. An Organisation with a Memory. London: Department of Health; 2000. Jeffries, P. R. (2005). A framework for designing, implementing and evaluating: Simulations used as teaching strategies in nursing. Nursing Education Perspectives, (2), 96-103. National Patient Safety Agency [www.npsa.org.uk]. Roopnarinesingh, S., Ramoutar, S & Bassaw, B.Maternal mortality at Mt Hope Women’s hospital, Trinidad. 1991. West Indian Medical Journal. Sept; 40(3): 139-41. World Health Organization. Beyond the Numbers; Reviewing Maternal Deaths and Disabilities to Make Pregnancy Safer. Geneva: WHO; 2004 [www.who.int/reproductive-health].