Download
1 / 27
310 likes | 604 Views
Insulin Dosing. Pattern Management. Jennifer Berry December 2013. Objectives. To understand the principles of pattern management To increase confidence in initiating and titrating basal insulin To increase confidence in initiating mixed insulin

E N D
Insulin Dosing Pattern Management Jennifer Berry December 2013
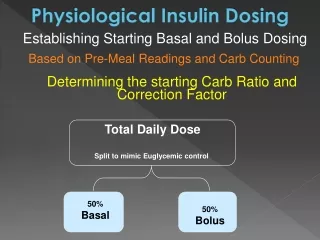
Objectives To understand the principles of pattern management To increase confidence in initiating and titrating basal insulin To increase confidence in initiating mixed insulin To increase confidence in initiating and titrating bolus insulin
BASAL INSULIN • NPH, Lantus, Levemir • “Bedtime Insulin” • “Long Acting” BOLUS INSULIN • Apidra, Humalog, Novorapid • “Mealtime Insulin” • Rapid Insulin BASAL-BOLUS • Rapid insulin PLUS Long acting insulin PREMIXED INSULIN • NovoMix 30, Novolin 30/70, Humalog Mix25 • Mix of rapid or short acting with intermediate insulin Insulin Options
Case Study: Jessica • Jessica is a 54 year old woman came to see you with an A1c of 8.2%. • SMBG: FBG 5.2 – 7.1 Bedtime 9.0 – 12.0 • Meds: • metformin 1000 mg twice daily • sitagliptin 100 mg daily • gliclazide MR 120 mg daily. • Lantus 50 units What is your next step?
Method 1. Sequential addition of bolus doses Fix the FPG first usual basal insulin Goal: FPG 4 to 7 mmol/L Consider adding bolus insulin when: A1c > 7% and FPG at goal or basal insulin dose > 0.5 units/kg Add bolus 4 units at largest meal Titrate to next pre-prandial (or bedtime) goal daily If subsequent pre-meal glucoses are: < 4 mmol/L : - 1 unit 4 to 7 mmol/L : Same dose > 7 mmol/L: + 1 unit Discontinue SU on addition of bolus insulin Get your patients to do the work. Teach them self-titration! If A1c > 7% after 3 months despite titrating bolus dose, or bolus dose is more than 30 units per meal: Add 2nd bolus of 4 units at 2nd largest meal and titrate as before. Repeat for 3rd bolus dose at final meal of the day Adapted from Nathan D. Diabetes Care 2008;32:193
Method 2. Straight to three boluses Fix the FPG first usual basal insulin Goal: FPG 4 to 7 mmol/L Consider adding bolus insulin when: A1c > 7% and FPG at goal or basal insulin dose > 0.5 units/kg Add bolus 2 units at each meal Titrate to next pre-prandial (or bedtime) goal daily If subsequent pre-meal glucoses are: < 4 mmol/L : - 1 unit 4 to 7 mmol/L : Same dose > 7 mmol/L: + 1 unit Discontinue SU on addition of bolus insulin. Patients need to monitor up to 4x/day Get your patients to do the work. Teach them self-titration! If A1c > 7% after 3 months despite titrating bolus dose, or bolus dose is more than 30 units per meal: Resume titration of basal insulin and/or consider performing a 7 point profile Adapted from Nathan D. Diabetes Care 2008;32:193
Jacob (Age 58) Meds: Metformin 1g BID Diamicron MR 120mg Januvia 100mg Lantus 58 units at Hs A1C 9.1% What is the next step?
Method 1. Sequential addition of bolus doses Fix the FPG first usual basal insulin Goal: FPG 4 to 7 mmol/L Consider adding bolus insulin when: A1c > 7% and FPG at goal or basal insulin dose > 0.5 units/kg Add bolus 4 units at largest meal Titrate to next pre-prandial (or bedtime) goal daily If subsequent pre-meal glucoses are: < 4 mmol/L : - 1 unit 4 to 7 mmol/L : Same dose > 7 mmol/L: + 1 unit Discontinue SU on addition of bolus insulin Get your patients to do the work. Teach them self-titration! If A1c > 7% after 3 months despite titrating bolus dose, or bolus dose is more than 30 units per meal: Add 2nd bolus of 4 units at 2nd largest meal and titrate as before. Repeat for 3rd bolus dose at final meal of the day Adapted from Nathan D. Diabetes Care 2008;32:193
Jacob Returns 3 Months Later Meds: Metformin 1g BID A1C 8.1% Lantus 58 units at Hs Apidra 12 units at supper What do you think of the FBG? Which insulin is responsible for this BG? What do you think of the Hs BG? Which insulin is responsible for this BG?
ALWAYS LOOK BACK… Look back to Hs Insulin Look back to lunch Insulin Look back to Bkft Insulin Look back to Supper Insulin Breakfast Lunch Supper Bedtime BLOOD SUGAR READING
Jacob Returns 3 Months Later(Con’t) Meds: Metformin 1g BID A1C 8.1% Lantus 58 units at Hs Apidra 12 units at supper What is your next step?
Method 1. Sequential addition of bolus doses Fix the FPG first usual basal insulin Goal: FPG 4 to 7 mmol/L Consider adding bolus insulin when: A1c > 7% and FPG at goal or basal insulin dose > 0.5 units/kg Add bolus 4 units at largest meal Titrate to next pre-prandial (or bedtime) goal daily If subsequent pre-meal glucoses are: < 4 mmol/L : - 1 unit 4 to 7 mmol/L : Same dose > 7 mmol/L: + 1 unit Discontinue SU on addition of bolus insulin Get your patients to do the work. Teach them self-titration! If A1c > 7% after 3 months despite titrating bolus dose, or bolus dose is more than 30 units per meal: Add 2nd bolus of 4 units at 2nd largest meal and titrate as before. Repeat for 3rd bolus dose at final meal of the day Adapted from Nathan D. Diabetes Care 2008;32:193
Jacob Returns 6 Months Later Meds: Metformin 1g BID A1C 6.9% Lantus 60 units at Hs Apidra 10 units at breakfast Apidra 14 units at supper Where to start looking first? (remember the cheat sheet)
Use 4 Principles For Pattern Management: Look for Lows FIRST What did the patient do / activity? What did the patient eat? What did the patient take? REMEMBER TO ALWAYS LOOK BACK…
Jacob – Identify Patterns Meds: Metformin 1g BID A1C 6.9% Lantus 60 units at Hs Apidra 10 units at breakfast Apidra 14 units at supper Where to start looking first? (What is most dangerous?) What is the next step? Remember to always look back…
Mary Lou (Ag3 65)Identify Patterns Meds: Metformin 1g BID A1C 7.9% Levemir 60 units at Hs Novorapid 40 units at breakfast Novorapid 40 units at lunch Novorapid 60 units at supper Where to start looking first? Remember principles What did the patient do / activity? What did the patient eat? What did the patient take?
IDENTIFY THE CAUSEBlood Glucose Overnight/ Before Breakfast HIGH LOW • Bolus insulin: Not enough before supper? • Basal insulin: Not enough at bedtime? • Somogyi Effect (Rebound hyperglycemia from excess basal? • Meal: Late supper? • Snack: Excess carbohydrate at bedtime snack? • Activity: Less than usual the day before? • Basal Insulin: Excess insulin before bed? • Meal: Early supper? • Snack: No bedtime snack? Or not have enough carbohydrates in the bedtime snack? • Alcohol consumption in the evening? • Activity: More than usual, longer duration of physical activity
Mary Lou– Identify Patterns Meds: Metformin 1g BID A1C 7.9% Levemir 60 units at Hs Apidra 40 units at breakfast Novorapid 40 units at lunch Apidra 60 units at supper What next? Anything look unusual? Remember principles What did the patient do / activity? What did the patient eat? What did the patient take?
IDENTIFY THE CAUSEBlood Glucose After Supper / Bedtime HIGH LOW • Bolus Insulin: Not enough before supper? • Meal: Excess carbohydrates at supper? • Activity: Less than usual daily activity? • Bolus insulin: Excess insulin before supper? • Meal: Missed supper? Or not have enough carbohydrates? • Activity: More than usual daily activity?
Mary Lou– 3 month follow up Meds: Metformin 1g BID A1C 6.1% Levemir 58 units at Hs Apidra 58 units at breakfast Novorapid 40 units at lunch Apidra 60 units at supper What to address first? Remember principles What did the patient do / activity? What did the patient eat? What did the patient take? Always look back…
IDENTIFY THE CAUSEBlood Glucose Before Lunch HIGH LOW • Bolus Insulin: Not enough before breakfast? • Meal: Excess carbohydrates at breakfast? • Timing of Meal: Was breakfast late / close to lunch? • Snack: Excess carbohydrates in the mid-morning snack? Or is it not required? • Activity: Less than usual morning activity? • Bolus insulin: Excess insulin before breakfast? • Meal: Missed breakfast? Or not have enough carbohydrates? • Timing of Meal: Was breakfast early and/or was lunch late? • Snack: No mid-morning snack? Or not enough carbohydrates in the morning snack? • Activity: More than usual morning activity
Mary Lou– Identify Patterns Meds: Metformin 1g BID A1C 7.9% Levemir 60 units at Hs Apidra 40 units at breakfast Novorapid 40 units at lunch Apidra 60 units at supper What next? Remember principles What did the patient do / activity? What did the patient eat? What did the patient take?
Switching from Premixed insulin to Basal Bolus Therapy • Calculate total daily dose on premixed insulin • e.g., premix 30 units bid = 60 units TDD • Calculate basal insulin dose as 50% of TDD • e.g. glargine, levemir, NPH = 50% of 60 units = 30 units • Calculate bolus insulin dose as 50% of TDD • e.g. aspart, lispro, glulisine = 50% of 60 units = 30 units • Divide as three equally divided doses before meals = 10 units before meals
Key points • Fix lows and fasting blood sugars first • Basal insulin is best targeted to ac breakfast sugars but will also help to bring down sugars throughout the rest of the day • Discontinue secretagogues with the addition of mealtime insulin • Use 3 principles for pattern management: • What did the patient do / activity? • What did the patient eat? • What did the patient take?