Download
1 / 46
700 likes | 1.61k Views
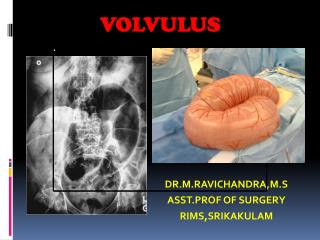
Sigmoid Volvulus. Volvulus describes the condition in which the bowel becomes twisted on its mesenteric axis This results in partial or complete obstruction of the bowel lumen and a variable degree of impairment of its blood supply. The condition most commonly affects the colon.

E N D
Volvulus describes the condition in which the bowel becomes twisted on its mesenteric axis • This results in partial or complete obstruction of the bowel lumen and a variable degree of impairment of its blood supply. • The condition most commonly affects the colon.
Any portion of the large bowel can torse if that segment is attached to a long and floppy mesentery that is fixed to the retroperitoneum by a narrow base of origin. • However, the mesenteric anatomy is such that volvulus is most common in the sigmoid colon, with less frequent occurrences involving the right colon and terminal ileum (usually referred to as cecalvolvulus), the cecum alone (the condition permitted by a highly mobile cecum, called a cecal bascule, that is mobile in a caudad to cephalad direction), and most rarely, the transverse colon.
ETIOLOGY • Sigmoid volvulus accounts for two thirds to three fourths of all cases of colonic volvulus. • The condition is permitted by an elongated segment of bowel accompanied by a lengthy mesentery with a very narrow parietal attachment, • This allows the two ends of the mobile segment to come close together and twist around the narrow mesenteric base.
ETIOLOGY (CONTD) • Associated factors include chronic constipation and aging, with the average age of presentation being in the seventh to eighth decade of life. • There is an increased incidence of the condition in institutionalized patients afflicted with neuropsychiatric conditions and treated with psychotropic drugs. • These medications may predispose to volvulus by affecting intestinal motility. • The increased incidence of volvulus in Third World countries has been attributed to a diet high in fiber and vegetables.
CLINICAL FEATURES • Sigmoid volvulus may present as acute or subacute intestinal obstruction with signs and symptoms indistinguishable from those caused by cancer of the distal colon. • There is usually a sudden onset of severe abdominal pain, vomiting, and obstipation. • The abdomen is usually markedly distended and tympanitic, with the distention often more dramatic than would be associated with other causes of obstruction.
CLINICAL FEATURES (CONTD…) • There is always the possibility that the condition can be associated with ischemia caused either by mural ischemia associated with the increased tension of the distended bowel wall or by arterial occlusion caused by torsion of the mesenteric arterial supply; therefore, severe abdominal pain, rebound tenderness, and tachycardia are ominous signs. • There may be a history of previous episodes of acute volvulus that spontaneously resolved, and in such circumstances, marked abdominal distention may occur with minimal tenderness
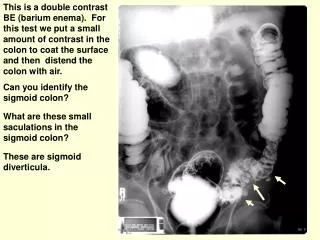
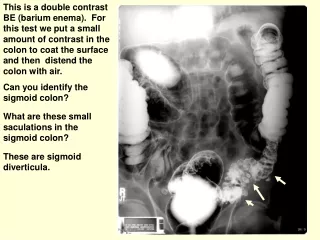
INVESTIGATIONS • They usually reveal a markedly dilated sigmoid colon with the appearance of a bent inner tube with its apex in the right upper quadrant. • An air-fluid level may be seen in the dilated loop of colon, and gas is usually absent from the rectum.
INVESTIGATIONS (CONTD…) • CT reveals a characteristic mesenteric whorl, although the diagnosis can usually be established on the basis of the clinical presentation and the plain film of the abdomen . • A contrast enema typically demonstrates the point of obstruction with the pathognomonic “bird's beak” deformity revealing the twist that obstructs the sigmoid lumen
TREATMENT • Treatment of the sigmoid volvulus begins with appropriate resuscitation and in most cases involves nonoperative decompression. • Decompressionrelieves the acute problem and allows resection as an elective procedure, which can be accomplished with reduced morbidity and mortality. Patients with signs of colonic necrosis are not eligible for nonoperative decompression. • Decompression can occur by placement of a rectal tube through a proctoscope or the use of a colonoscope. • Often, a soft rectal tube can be inserted under direct vision through the twist of the volvulus while the patient is in the emergency room. • Decompression results in a sudden gush of gas and fluid, with a decrease in the abdominal distention.
TREATMENT (contd) • The reduction should be confirmed with an abdominal radiograph. • The rectal tube should be taped to the thigh and left in place for 1 or 2 days to allow continued decompression and to prevent immediate recurrence of the volvulus. • The bowel can then be cleansed with cathartics and a complete colonoscopic examination performed. • If a rectal tube cannot be passed as described, detorsion of the volvulus with the colonoscope should be attempted. • If detorsion of the volvulus cannot be accomplished with either a rectal tube or colonoscope, laparotomy with resection of the sigmoid colon (Hartmann's operation) is required.
Even if detorsion of the sigmoid is successful, elective sigmoid resection is indicated in most cases because of the extremely high recurrence rate (approaching 50%). • The operation can be conducted through a small left lower quadrant incision or by a laparoscopic approach. • Because the elongated colon and mesentery require virtually no mobilization, resection with primary anastomosis is easily accomplished. • Colonoscopy should be performed before elective resection to exclude an associated neoplasm
Although the term cecalvolvulus is ingrained in the literature, true volvulus of the cecum probably never occurs. • There is a well-recognized condition in which the cecum folds in a cephalad direction anteriorly over a fixed ascending colon. • Although gangrene may develop, this is exceedingly rare because there is not major vessel obstruction. • This so-called cecal bascule commonly causes intermittent bouts of abdominal pain because the mobile cecum permits intermittent episodes of isolated cecal obstruction that are spontaneously relieved as the cecum falls back into its normal position.
The condition commonly referred to as cecalvolvulus is actually a cecocolicvolvulus and consists of an axial rotation of the terminal ileum, cecum, and ascending colon with concomitant twisting of the associated mesentery. • This is a relatively rare condition • Cecocolicvolvulus is possible because of a lack of fixation of the cecum to the retroperitoneum. • Factors that have been implicated in causing a cecalvolvulus include previous surgery, pregnancy, malrotation, and obstructing lesions of the left colon. • Cecocolicvolvulus is somewhat more common in women, whereas sigmoid volvulus occurs with equal frequency in both sexes. Cecocolicvolvulus affects a younger age group (most common in the late 50s) than sigmoid volvulus.
The typical presentation of patients with cecocolicvolvulus is the sudden onset of abdominal pain and distention. • In the early phases of a cecocolicvolvulus, the pain is mild or moderate in intensity. If the condition is not relieved and ischemia occurs, the pain increases significantly. • Physical examination may reveal asymmetric distention of the abdomen, with a tympanitic mass palpable in either the left upper quadrant or midabdomen.
Plain radiographs of the abdomen reveal a dilated cecum that is usually displaced to the left side of the abdomen. • The distended cecum usually assumes a gas-filled comma shape, the concavity of which faces inferiorly and to the right. • Occasionally the distended cecum appears as a circular shape with a narrow, triangular density pointing superiorly and to the right. • Haustral markings in the distended loop indicate that the dilated bowel is colon. The torsion results in obstruction of the small bowel, and the radiographic pattern of dilated small intestine can cause diagnostic difficulty. • If ischemia has already occurred, immediate operation is obviously required. Contrast enema is helpful to con-firm the diagnosis and to exclude a carcinoma of the distal bowel as a precipitating cause of the volvulus
Right colectomy is the procedure of choice. • Primary anastomosis is usually preferred unless the volvulus has resulted in frankly gangrenous bowel, in which case resection of the gangrenous bowel with ileostomy is a safer approach. • There have been many reports of correcting cecocolicvolvulus with cecopexy, which should avoid the complication associated with an anastomosis. • However, the operation to provide fixation of the cecum is extensive and entails elevating and attaching a flap of peritoneum over the surface of the cecum and ascending colon. • The recurrence rates are high with cecopexy, and right colectomy remains the procedure of choice for most surgeons.
Volvulus of the transverse colon is extremely rare and tends to be associated with other abnormalities such as congenital bands, distal obstructing lesions, and pregnancy. • Clinical features are indistinguishable from other causes of large bowel obstruction. • Radiologic examination is not particularly useful because many cases are misdiagnosed as sigmoid volvulus. • A contrast study may show a bird's beak deformity indicating a volvulus. In such cases, colonoscopic reduction may result in detorsion and relief of obstruction. • Elective resection should follow to prevent recurrence
Polyp is a swelling arising from the mucosal surface with a pedicle. • ‘Poly’ means many • Polyp is a mass projecting into the bowel lumen beyond the surface epithelium
CLASSIFICATION INFLAMMATORY • Ulcerative colitis • Segmental colitis • Crohn’s disease • Diverticulitis • Dysentric Colitis HYPERPLASTIC • Metaplastic mucosal polyps
HAMARTOMATOUS • Peutz-Jegher’s syndrome • Juvenile polyp • Cronkhite – Canada syndrome NEOPLASTIC • Tubular- pedunculated • Villous- sessile • Tubulo- villous • FAP- Familial Adenomatouspolyposis OTHERS • Lipoma, hemangioma, leiomyoma
JUVENILE POLYPS • Commonest polyp of the colorectum in infants & childern • Can cause intussusception, prolapse through rectum, bleeding • Colonoscopicpolypectomy is done • Not a premalignant condition
METAPLASTIC /HYPERPLASTIC POLYPS • Metaplastic- indicates a different appearance from a normal mucosa • Very small in size – 1 to 2 mm • Multiple • Common in the rectum • Also occurs in other parts of the rectum • Contains columnar epithelium, cystic dilatation, goblet cells & lymphocytes • Not a pre malignant condition
PEUTZ-JEGHER’S POLYP • Common in small intestine(jejunum) but can also occur in large intestine • They are multiple, familial, hamartomatousintestinal polyps • Associated with melanosis of oral mucosa, lips, & occasionally digits • Microscopically it contains tree like branching filaments of the mucosa with smooth muscle wall • It is an autosomal dominant disease with germline defect in suppressor threoninekinase 11
COMPLICATIONS • Bleeding or intussusception when occurs requires surgery either resection – anastamosis or colonoscopic removal
ADENOMA OF COLON • Can be tubular, villous, tubulovillous • Tubular is the commonest • It can be solitary or multiple, sessile or pedunculated • Tubular is commonly 1-2mm sized & sessile is 3-4 mm sized
It has malignant potential • Potentially increase with size – • Size is an important factor in causing carcinoma • Sessile nature • Villous architecture • dysplasia
GRADING OF ADENOMA • I – Minimal hyperplasia,no cellular atypia • II- Mild hyperplasia, cellular atypia • III- Moderate hyperplasia, cellular atypia • VI- Severe hyperplasia, cellular atypia • V- Carcinoma in situ
FEATURES OF ADENOMA • Can be asymptomatic • Bleeding per annum is usually chronic but rarely can be acute • Anaemia • Prolapse – common in tubular type • Diarrhea common in villous type • Tenesmus, colicky abdominal pain • Spurious diarrhea • Poor general health • Electrolyte imbalance– hypokalemia • Carcinomatous changes
INVESTIGATIONS • Serum electrolytes • Barium enema – multiple filling defects • Colonoscopy biopsy :- • Size should be noted • Texture – harder tumor more likely to be malignant • Color – pale is benign, pink, red & active could be carcinoma • Ulceration on the surface if it has turned malignant
TREATMENT • Colonoscopicpolypectomy using snare. Any adenoma more than 5mm in size should be removed • Diathermy excision/coagulation with sigmoidoscope • Per anal polypectomy • Per-anal excision with clear margin of the rectal sessile adenoma • Open abdominal colotomy & polypectomy in case of huge adenoma • Segmental resection of the colon if polyps/adenomas are restricted to one segment of colon • Total colectomy/proctocolectomy if multiple polyps present all over colorectum & if associated with FAP
DEFINITION An autosomal dominantly inherited syndrome characterized by hundreds to thousands of adenomatous polyps throughout the colorectum and a variety of extracolonic manifestations such as upper gastrointestinal polyps(gastric,duodenal,periampullary),desmoids and retinal lesions.
APC mutations arethe earliest eventin the development of the tumor
Risk of Colorectal Cancer (CRC) 5% General population Personal history of colorectal neoplasia 15%–20% Inflammatory bowel disease 15%–40% 70%–80% HNPCC mutation >95% FAP 0 20 40 60 80 100 Lifetime risk (%)
SURGERY RESTORATIVE PROCTOCOLECTOMY WITH AN ILEOANAL POUCH (Parks) • A pouch is made out of ileum as a substitute for rectum & sewn to the anal canal • The different pouch designs are J Pouch, S Pouch & W Pouch • Frequency of evacuation is determined by the pouch volume
Sometimes a temporary Ileostomy is done • Complications like pelvic abscess, post operative small bowel obstruction can occur • Although mucosectomy of upper anal canal with an anastamosis at the dentate line is claimed to remove all of the at risk mucosa & any problem of subsequent cancer , it may also increase the risk of incontinence with nocturnal seepage