Download
1 / 18
300 likes | 1.16k Views
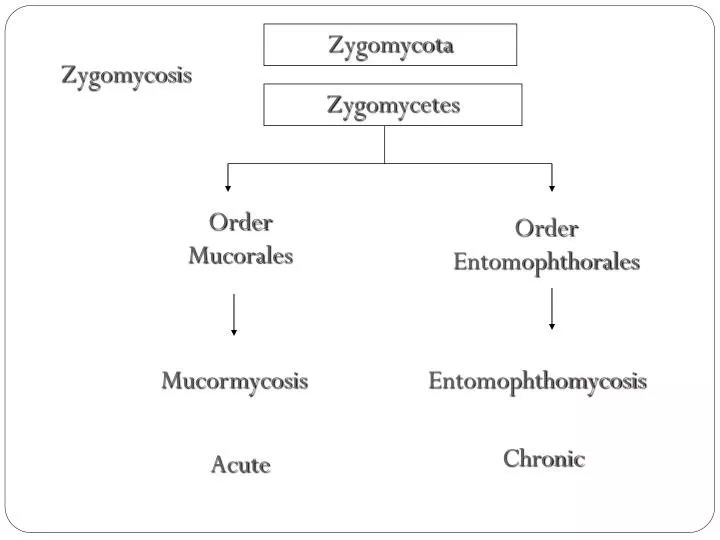
Zygomycota. Zygomycosis. Zygomycetes. Order Mucorales. Order Entomophthorales. Mucormycosis. Entomophthomycosis. Chronic. Acute. Mucorales infections Definition . Angiotropic (blood vessel-invading) The most common genera causing disease are: Rhizopus Absidia Mucor Rhizomucor

E N D
Zygomycota Zygomycosis Zygomycetes OrderMucorales Order Entomophthorales Mucormycosis Entomophthomycosis Chronic Acute
Mucorales infectionsDefinition • Angiotropic (blood vessel-invading) • The most common genera causing disease are: • Rhizopus • Absidia • Mucor • Rhizomucor • Fast growing non-septate molds
Clinical forms • The infection typically involves the: • Rhino-facial-cranial area • Lungs, gastrointestinal tract or skin • Other parts can also be affected
Risk factors • The disease is associated with: • Diabetic ketoacidosis • Malnourished children • Severely burned patients • It is also seen in immunocompromised patients: • Leukemia • Lymphoma • AIDS • In patients using corticosteroids
Invasive zygomycosis A 45-year-old woman with poorly controlled diabetes mellitus with facial and periorbital swelling due to zygomycosis. Author: Jose A Vazquez, MD, Associate Professor, Department of Internal Medicine, Division of Infectious Diseases, Wayne State University School of Medicine
Entomophthorales infections • Causes subcutaneous zygomycosis • Tow genera are involved: • Conidiobolus • Basidiobolus
Entomophthorales infections • Infections are: • Chronic • Slowly progressive • Restricted to the subcutaneous tissue • Not like Mucorales: • No vascular invasion or infarction
Basidiobolus infection • Chronic inflammatory or granulomatous disease • Subcutaneous tissue of the limbs, chest, back or buttocks • Mostly in children (predominance in males)
Conidiobolus infection • Chronic inflammatory or granulomatous disease • Nasal submucosa • Characterized by polyps or palpable subcutaneous masses • Occur mainly in adult (80% of cases)
Zygomycosis caused by Basidiobolusranarum Zygomycosis caused by Conidiobolus
Laboratory diagnosis • Specimens: • Aspirated material from sinuses • Sputum in pulmonary disease • Biopsy material • 10 or 20% KOH: • Typically contain thick-walled aseptatehyphae • Swollen cells (up to 50 um) and distorted hyphae may be present
Zygomycosis Tissue sections stained with PAS
Laboratory diagnosis (continued) • Culture: • SDA without cycloheximide at 30°C • Characterized by rapid growth
Absidia Rhizomucor
Management of mucormycosis • The prognosis is bad • Most cases of gastric and pelvic disease are diagnosed at autopsy • Cases occurred in patients with pulmonary disease, leukemia, or with lymphomas, are usually fatal • Control of the diabetes, aggressive surgical debridement of involved tissue, and high doses of Amphotericin B are recommended
Management of Entomophthoromycosis • Infections caused by Basidiobolus • Drug of choice saturated potassium iodide solution for 6-12 months • Oral ketoconazole and fluconazole • Sub-mucosal infections caused by Conidiobolusspecies: • Potassium iodide solution • Amphotericin B • Trimethoprim-sulfamethoxazole