Download
1 / 1
10 likes | 139 Views
THE ANATOMIC CONSEQUENCES OF ARTHROSCOPIC CORACOPLASTY: AN ANATOMIC DISSECTION STUDY Aruna Seneviratne, MD; Ken Montgomery, MD; Babette Bevilacqua, PAC; Bashir A Zikria, MD Lenox Hill Hospital, New York, NY, USA. CAL - Coraco-acromial Ligament

E N D
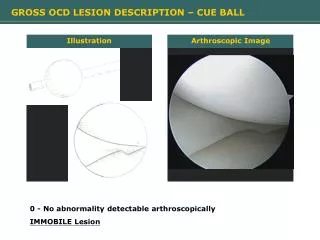
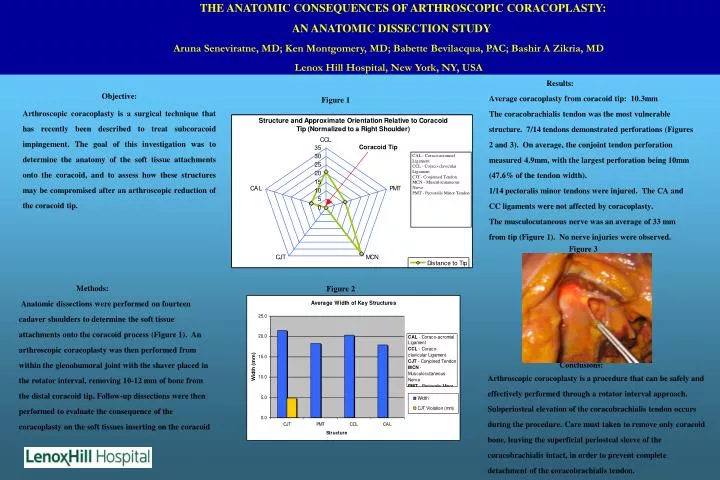
THE ANATOMIC CONSEQUENCES OF ARTHROSCOPIC CORACOPLASTY: AN ANATOMIC DISSECTION STUDY Aruna Seneviratne, MD; Ken Montgomery, MD; Babette Bevilacqua, PAC; Bashir A Zikria, MD Lenox Hill Hospital, New York, NY, USA CAL - Coraco-acromial Ligament CCL - Coraco-clavicular Ligament CJT - Conjoined Tendon MCN - Musculocutaneous Nerve PMT - Pectoralis Minor Tendon Figure 3 Results: Average coracoplasty from coracoid tip: 10.3mm The coracobrachialis tendon was the most vulnerable structure. 7/14 tendons demonstrated perforations (Figures 2 and 3). On average, the conjoint tendon perforation measured 4.9mm, with the largest perforation being 10mm (47.6% of the tendon width). 1/14 pectoralis minor tendons were injured. The CA and CC ligaments were not affected by coracoplasty. The musculocutaneous nerve was an average of 33 mm from tip (Figure 1). No nerve injuries were observed. Objective: Arthroscopic coracoplasty is a surgical technique that has recently been described to treat subcoracoid impingement. The goal of this investigation was to determine the anatomy of the soft tissue attachments onto the coracoid, and to assess how these structures may be compromised after an arthroscopic reduction of the coracoid tip. Figure 1 Methods: Anatomic dissections were performed on fourteen cadaver shoulders to determine the soft tissue attachments onto the coracoid process (Figure 1). An arthroscopic coracoplasty was then performed from within the glenohumoral joint with the shaver placed in the rotator interval, removing 10-12 mm of bone from the distal coracoid tip. Follow-up dissections were then performed to evaluate the consequence of the coracoplasty on the soft tissues inserting on the coracoid Figure 2 Conclusions: Arthroscopic coracoplasty is a procedure that can be safely and effectively performed through a rotator interval approach. Subperiosteal elevation of the coracobrachialis tendon occurs during the procedure. Care must taken to remove only coracoid bone, leaving the superficial periosteal sleeve of the coracobrachialis intact, in order to prevent complete detachment of the coracobrachialis tendon.