Download
1 / 47
882 likes | 1.78k Views
The New Zealand Health and Disability System. Anthony Hill Deputy Director-General Ministry of Health. Contents. Overview New Zealand Public/Private in New Zealand Public Health and Disability System Issues Pressures facing the system Strategies Government priorities

E N D
The New Zealand Health and Disability System Anthony Hill Deputy Director-General Ministry of Health
Contents • Overview • New Zealand • Public/Private in New Zealand • Public Health and Disability System • Issues • Pressures facing the system • Strategies • Government priorities • Examples of changes • Primary Health • Service Configuration • Elective Services • Pharmaceutical Management Agency (PHARMAC) • Shared Services Agency • Health Workforce New Zealand • Health Quality and Safety Commission
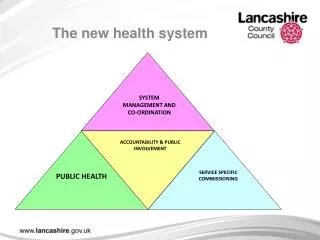
Contents • Overview • New Zealand Health and Disability System • Issues • Strategies
1,313,100 3.4m 197,300 381,900 1.0m 382,200 114,900 New Zealand population Current Total: 4,365,600 Figures for estimated resident population at 30 June 2008: city totals are for urban areas; source Statistics NZ.
The Treaty of Waitangi 1840 • Partnership • Participation • Protection
The New Zealand Health and Disability System Predominantly publicly funded system (from general taxation) • taxes on the basis of our income • provision of comprehensive health services for all System results: - free hospital care for all New Zealanders; - substantial public funding/subsidies for primary healthcare; - most hospitals are publicly owned; - private hospital sector is largely for people with private health insurance (or willing to pay), who want to receive early care without waiting; - primary care is operated by private providers with subsidies available for patients; - specialists can work in both the public and private system (greater remuneration to retain workforce). Extremely cost effective system (8.5% of GDP) - delivers good and necessary care for most people in a timely way
Public/Private • Government • Public funding services is about 78% of health care costs: taxation (86%), levies on employers (13%) and local government (1%) • Enduring public preferences (eg. 80% public funding; NZ’s particular mix of public and private providers; equity matters) • Private insurance • About one third of NZers have private health insurance; it covers 6% of total health care expenditures (2008) eg, for elective surgery in private hospitals • Out of Pocket payments • account for 16% of total health care expenditure (2008): patient co-payments for General Practitioner services, pharmaceuticals; private hospital/ specialist care, or adult dental care • Coverage for accidents and injury is for everyone • financed by a separate quasi-government organisation (Accident Compensation Corporation)
Private Market • Private total 22% in 2007/08 • Out of Pocket -16% • Insurance - 5% • Not-for-profit organisations – 0.9% • Private Provision • Private Hospitals • General Practitioners (component not subsidised) • Long Term Care • Home Care • Private Specialists • Non-Profit Organisations • Disability support • Palliative care
Sources of Funding Source: Health Expenditure Trends in New Zealand, 1996–2006, Ministry of Health, 2008
Public Funding • Population Based Funding Formula (PBFF) • Aggregate formula to determine the share of funding to be allocated to different districts across New Zealand • Based on the population living in each district: • Size of population • Age, sex, ethnicity, socio-economic and unmet needs adjustments • Rural adjustments • Overseas visitors adjustment
Pricing Mechanisms • Provider Payments • Population Based Funding Formula • Crown Funding Agreements • Inter-District Flows • Pricing (National Pricing Programme) • joint Ministry of Health/District Health Board programme • purchase units for an agreed price • average costs of services • tertiary and efficiency adjustor
How does the system rank? $$ per person Life expectancy at birth
Contents • Overview • New Zealand Health and Disability System • Issues • Strategies
Pressures Demandpressures Supply pressures • Demographic changes • Workforce constraints • Long-term conditions • Unsustainable funding growth • Health inequalities • New technologies • Public expectations
Particular Pressures – Health of Older People • ~ 580,000 people in New Zealand are aged over 65 (13% of the population) • 2009/10 - 35% of public health spending was on people aged 65+ • Expected 85% increase in the population of people over 65 in 20 years (to 1 million) • Key numbers: $4-6 billion will be required for new investments before 2026 ($275 million per year) • For comparison – 2.5% of public money needed for residential building investments in the economy and 10% of the expenditure on roads
Age Distribution of Population Statistics New Zealand, March 2006
Particular Pressures - Obesity Data: OECD Health Data 2006-2008
85 80 European females 75 Pacific females life expectancy at birth (years) European males 70 Pacific males Māori females 65 Māori males 60 1 2 3 4 5 6 7 8 9 10 NZ Deprivation scale Life Expectancy by Ethnicity and Deprivation
Contents • Overview • New Zealand Health and Disability System • Issues • Strategies
New Government was elected in 2008 with a strong health policy agenda • Better, Sooner, More Convenient: clear policy focus on strengthening services • Priorities: electives; hospital productivity; clinical leadership; workforce; primary care • Need for long term sector plan identified • Global fiscal crisis: ‘the future is now’
Two major initiatives Ministerial Review Group “Meeting the Challenge” • Independent Review • Recommendations: • Establishment of National Health Board • Improved Regional/ National/ Local decision making • Quality Agency • Prioritisation • Legislative change 100 Day Action Plan • Halt the growth in health bureaucracy • Elective Services • Plunketline • 12-month course of Herceptin • National's Tackling Waiting Lists plan • Voluntary Bonding Scheme
Examples of changes to the system • Primary Health • Service Configuration • Elective Services • Pharmaceutical Management Agency (PHARMAC) • Shared Services Agency • Health Workforce New Zealand • Health Quality and Safety Commission
1. Primary Health Why focus on primary health? Countries with strong primary health care demonstrate: • improved population health outcomes • reduced health inequalities • and deliver this at lower cost Primary Health Care in New Zealand • Complex public/private partnership where District Health Boards contract (on behalf of the Crown) with Primary Health Organisations who contract with over 1,000 privately owned General Practitioner Practices
Meeting Primary Health Challenges • Primary Health Challenges • Health inequalities – access barriers, more chronic disease • Workforce shortages • Funding pressures • Safety and quality – unexplained variability in performance • Meeting the Challenges • Improving performance through practice accreditation and a Primary Health Organisation Performance Programme • Increasing access by reducing fees • Greater use of nurses • Focus on chronic care management
2. Service Configuration -Local / Regional / National • Increased collaboration to obtain efficiencies • Shared services around ‘ back office’ functions • Increased use of clinical networks • Vulnerable services • Clinical leadership
Trends in Models of Care & Service Design • How health service design is responding to the intensifying pressures of: • demand (demographics; long term conditions; health inequalities; public expectations) and • supply (workforce; funding; new technologies) • Review of New Zealand and international trends • Overall theme: • ‘Localise where possible, centralise where necessary’
3. Elective Services • Issue: long waiting lists for surgeries • Solution: separate elective care from the pressures of acute (emergency) care: • address issues in the National Booking and Reporting System and the Patient Management Systems • theatre utilisation • increase operating theatres ($180m over five years)
Bed Days and Potential Savings • In 2008/09 there were 1,587,000 hospital bed days across all Provider Arms • Analysis at DRG level (including population standardisation) reveals 136,000 bed days are in excess of sector averages • At marginal bed day costs, this is equivalent to $60M ($ 2008/09). If excess bed days were released to other patients, DHBs could serve 32,000 additional inpatients • As a percentage of total bed days, the percentage of excess bed days varies across DHBs from 4.7 to 14.9 percent • Of excess bed days, 72 percent are acute and 28 percent are elective/arranged • The bulk of excess bed days lies in a relatively narrow band of DRGs (and further investigation should therefore be feasible)
Theatre Utilisation • New Zealand provisional theatre data (2007/08) compared with Australian benchmarks. Considerable variation within peer groups, with few facilities matching benchmarks. • If the benchmarks had been matched, this would have equated to an additional 70,000 operations during 2007/08 (28 percent increase).
Outcomes? More surgical discharges
4. PHARMAC • What is PHARMAC? • agency of the New Zealand Government that decides which medicines to subsidise • balances the public’s growing demand for new medicines within a defined budget • What does PHARMAC do? • manages the Pharmaceutical Schedule of over 2000 Government-subsidised community medicines • promotes best possible use of medicines • manages the subsidy of some medicines and products for public hospitals • manages the Exceptional Circumstances schemes (medicines funding for people with rare conditions) and other special access programmes
Outcomes? • pharmaceutical expenditure growing second slowest in OECD
Future considerations for PHARMAC-like model • Effective model – can it be used of the procurement of medical devices, vaccinations and hospital medicines? • Government consulting with stakeholders on future possibilities
5. Shared Services Agency Background • 20 District Health Boards each with individual administration and support services • Examples of administration and support services include: • Information Technology • Food Preparation • Procurement of supplies
Shared Services Agency (continued) • Studies indicate substantial savings available by consolidating District Health Board administration and support services • Government keen to see all possible efficiencies in the public sector recognised • In May 2010 Cabinet determined to establish a Shared Services Agency as a company under the Public Finance Act
6. Health Workforce New Zealand • New Zealand faces an increasing demand for workers across the health and disability system • Workforce development activity previously fragmented, uncoordinated and driven by district needs • July 2009 - Clinical Training Agency board (later rebranded Health Workforce New Zealand board) was established as an interim measure to drive immediate change relating to workforce • Consolidation of health workforce activity into a Health Workforce New Zealand Business Unit in the Ministry of Health • Business Unit – oversees and drives the rationalisation of workforce planning, training and purchasing within the public health sector
Foreign Born Health Workforce Percentage of foreign-born doctors and nurses from selected OECD countries (Source: OECD. Health Workforce and International Migration: Can New Zealand Compete, 2007) Proportion of International Medical Grads between 1980 and 2008 (Source: Medical Council of New Zealand, The New Zealand Medical Workforce in 2008)
7. Health Quality and Safety Commission • Concerns about insufficient priority being given to quality and safety measures • Creation of a new separate quality and safety improvement agency, independent of the health system’s regulatory, funding and performance monitoring functions • December 2009 – Government agrees to establish the Commission, to perform the following functions: • public reporting of quality and safety indicators including, initially, serious and sentinel events • leading and coordinating work to improve quality and safety across the health and disability system • any other functions that it is authorised to perform by the Minister of Health by written notice after consultation with it, including the collection, analysis and dissemination of information. • Commission is to be established as a Crown agent under the Crown Entities Act
Summary • New Zealand’s health and disability system is cost effective and delivers good and necessary care for most people in a timely way • Mix of public and private provision • A number of pressures facing the system – particularly an increased number of people over 65, obesity and inequalities • Government has a number of strategies to address these: • Primary health • System reconfigurations • Elective services • Prioritisation • Efficiencies • Health workforce • Quality and safety
Grazie Associazione Italiana Ospedalità Privata!