Download
1 / 20
260 likes | 912 Views
Chapter 4 Asthma. Topics. Pathology of asthma Lung mechanics Gas exchange Airflow in the lung Convection and diffusion Airway resistance Breathing cycle Pathogenesis of asthma Bronchoactive drugs. Case Study #4: Debra. 30 yr old School teacher Asthma for 20 yrs Shortness of breath

E N D
Topics • Pathology of asthma • Lung mechanics • Gas exchange • Airflow in the lung • Convection and diffusion • Airway resistance • Breathing cycle • Pathogenesis of asthma • Bronchoactive drugs
Case Study #4: Debra • 30 yr old School teacher • Asthma for 20 yrs • Shortness of breath • Particularly in spring • Pollen • During exercise • Exposure to cold air
Case Study #4: Debra • Main complaint: SOB • Particularly in spring • Frequent attacks of wheezing • Cold air and exercise provoke her asthma • Stress also provokes asthma • Otherwise healthy
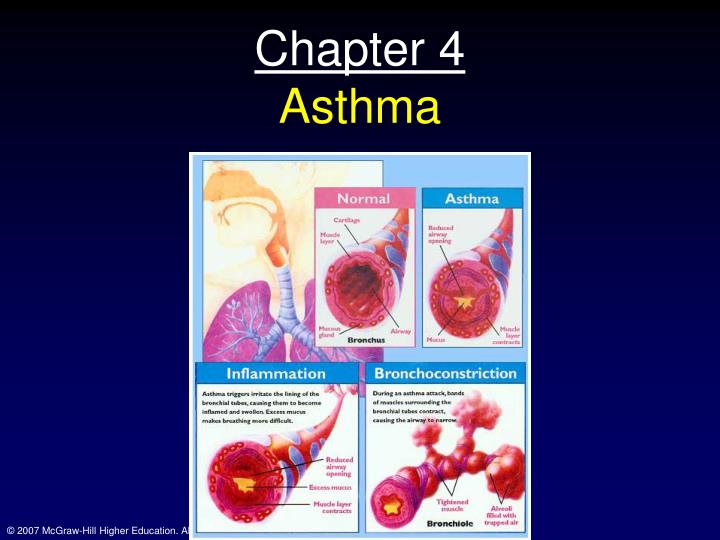
Pathology • Hypertrophied smooth muscle • Enhanced bronchoconstriction • Hypertrophied mucus glands • Bronchial inflammation and edema • Mucus plugs • Coughed up sputum (non-purulent)
Pulmonary function tests • During an attack, all indicesof expiratory flow are reduced significantly • FEV1.0 • FEV1.0/FVC • FEF25-75% • FVC reduced; why? • Usually responds well to bronchodilator; why?
Pulmonary function in asthma • Expiratory flow-volume loops also examined • Flow rates are reduced in asthma and EILV and EELV are increased • Compare to restrictive lung disease, where EILV and EELV are reduced
Pathology • During asthma • Lung volume is increased • FRC, TLC and RV all increased • Due to some loss of elastic recoil and premature closure of small airways • Due to inflammation, edema and increased smooth muscle tone
Gas exchange • Arterial hypoxemia common • Caused by VA/Q mismatching • Caused by uneven ventilation and also uneven blood flow, which is caused by hypoxic pulmonary vasoconstriction in regions of the lung where ventilation is greatly reduced • Bronchodilators may improve lung function while worsening hypoxemia (relief of VC in poorly ventilated airways) • However, the relief given (i.e. reduced perception of breathing effort) offset the drop in PaO2 at rest
Physiology & pathophysiology • Principle of airflow • Through tubes • Laminar flow: low flow rates • Transitional: as flow rates increase, at branch points, flow is no longer linear • High flow rates: turbulence; disorganized flow Laminar flow: Poiseuille’s law: V=(pπr4)/(8nl) P=ΔP; r=radius; n=viscosity and l=length
Physiology & pathophysiology • In laminar flow, the gas in the middle moves twice as fast as the average velocity; the friction of the sides of a tube slow down flow in those regions; flow rate is proportional to driving pressure: P=V; gas density has NO effect under these conditions. Greater ΔP, greater V • Turbulent flow: P=V2 in addition, gas density becomes more important here; P1-P2 is greater for a given flow as gas density increases; or greater ΔP necessary to achieve a given V as gas density increases Whether flow is laminar or not is dependent upon the Reynolds number: Re=(2rvd)/n R=radius, V=velocity and d=density, n=viscosity Turbulence likely when # exceeds 2000
Convection and diffusion in the airways • Convective flow and it’s attendent turbulence occurs in the conducting zone • In terminal and respiratory bronchioles gas moves primarily by diffusion • As the total cross sectional area increases flow rate is reduced • Because volume flow is the same and the number of airways and their combined cross-sectional area are increased • This is okay, because the distances are short and the diffusive resistance is small
Airway resistance and pressure cycles • Airway resistance: • R=(Pmouth-PA)/flow rate • R is the ration of ΔP to V • A: Lung volume inc during inspiration and decreases during expiration • B: Pleural pressure falls during insp. And rises during expiration • Always negative; why? • Asymmetrical profile due to the elastic recoil (dashed line) and changing alveolar press. So solid line is actual • C: Flow rate: increases during insp and exp; zero at transition • D: Alveolar pressure: mirrors flow rate
Sites of airway resistance • As airways divide throughout lung, they become more numerous and narrow • Where is the greatest resistance to flow? • As R=P/Q one might think the small airways because of the small radius • No, it’s the medium sized airways; why? • Laminar flow in terminal airways • P=V • Extremely large number of small airways • Each airway has high resistance, but since flow is spread out over sooo many airways, total resistance is small
Airway resistance • Bronchial smooth muscle • Bronchoconstriction • Reflexive; controlled by Vagus n.; Ach causes BC, sympathetic stim causes BD • Lung volume • Bronchial diameter inc. as lung vol inc. • Below a certain vol (closing vol.); resistance is so high that no flow occurs (conductance is zero)
Airway resistance • Gas density and viscosity effects • Impact the Reynold’s number and the resistance • Flow resistance increases during diving • Inc. gas density (inc. Reynold’s #) • Helium reduces density • Thus, these effects are mostly in medium sized bronchi where turbulence is most likely and resistance is highest and thus, can be changed the most
Uneven Ventilation • Phases of expiration and the gas content after single breath of oxygen • Phase one: rapid, pure O2 from upper airways • Phase 2: N2 rises rapidly, washout of anatomic DS • Phase 3: N2 plateaus, alveolar gas coming out • Slope is a measure of ventilatory inequality • Phase 4: onset is closing volume of lung; end is RV
Airway closure and uneven ventilation • Uneven ventilation in the lung • Partial obstruction of an airway • Series inequality • Dilation of peripheral air sacs • Emphysema • Collateral ventilation • Asthma • S lows emptying of closed units
Pathogenesis of Asthma • Airway hyperresponsiveness and inflammation • They are related • Triggers • Allergens • Cold, dry air • Pollution • Chemical mediators • Mast cells, WBCs • Histamine, Leukotrienes (and arachidonic acid), Bradykinin, cytokines (interleukins) • Prostaglandins, reactive oxygen species, etc.
Bronchoactive drugs • Β-adrenergic agonists • Two types of β receptors • β1 in heart, β2 in lung • Stimulation of β2 receptors • Relaxes smooth muscle in bronchi • Albuterol intermediate time course • Salmeterol long acting • Work through adenylate cyclase-cAMP pathway • Corticosteroids • Inhibit inflammatory/immune response • Enhance β-receptor expression and/or function • Methylxanthines (caffeine breakdown products) • Theophylline or aminophylline • Bronchodilatory and anti-inflammatory effects • Anticholinergics • Block parasympathetic system; usu in sever COPD • Cromolyn and nedocromil • Block inflammation, possibly through mast cell stabilizing effects • New therapies • Leukotriene anatagonists (singulair) and 5-lipoxygenase inhibitors (perhaps more effective with allergic asthma)