Download
1 / 44
470 likes | 702 Views
Intravenous GP IIb/IIIa Inhibitors. Abciximab (c7E3 Fab, ReoPro) = Human- murine chimeric monoclonal Fab antibody fragment Eptifibatide (Integrilin) = A cyclic heptapeptide based on the Lys-Gly-Asp (KGD) amino acid sequence

E N D
Intravenous GP IIb/IIIa Inhibitors • Abciximab (c7E3 Fab, ReoPro) = Human- murine chimeric monoclonal Fab antibody fragment • Eptifibatide (Integrilin) = A cyclic heptapeptide based on the Lys-Gly-Asp (KGD) amino acid sequence • Tirofiban (Aggrastat) = Tyrosine derivative non-peptide mimetic inhibitor
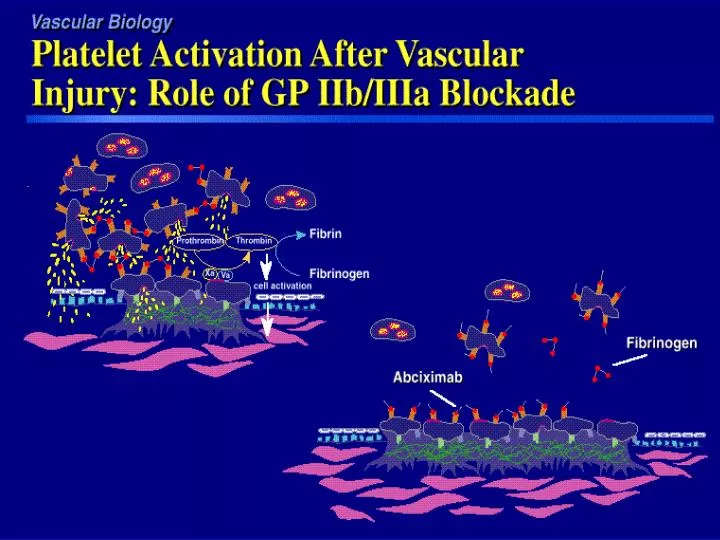
Intravenous GP IIb/IIIa InhibitorsAbciximab (ReoPro) • Has a rapid, high affinity to platelets within minutes • Dissociation slowly from GP IIb/IIIa receptor • Clears rapidly from plasma but remains bound to circulating platelets up to 21 days • Binding to IIb/IIIa receptor is non-specific and has equal affinity for the vitronectin receptor which appears to play a role in cell adhesion, migration and proliferation
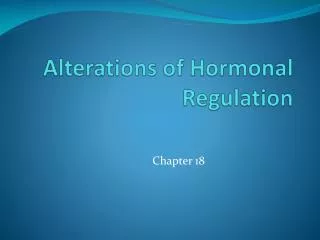
IV IIb/IIIa Inhibitors and Time course of Action on Platelets
N = 1265 N = 2099 N = 2792
EPISTENT Stent Placement Placebo/Stent Abx /Stent Abx /Balloon Placebo/Stent Abx /Stent Abx /Balloon No. Patients 809 794 796 No. Patients Stent Placed (%) 95.3 96.9 19.1 Stent Placed (%) No. Stents/Pt (%) No. Stents/Pt (%) 1 69.6 73.8 66.4 1 2 21.9 20.2 23.0 2 3 5.7 4.5 7.2 3 ³ ³ 2.7 1.6 4 3.3 4 Maximum Balloon Maximum Balloon Inflation Pressure (mm) 16.0 16.0 16.0 Inflation Pressure (mm)
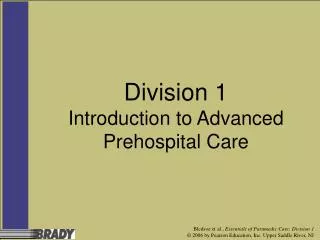
EPISTENT 1 Endpoint: Placebo/Stent Abciximab/Stent Abciximab/PTCA 15 12.1 12 10.8 9.2 9 6.8 Incidence (%) 6.4 5.3 6 3 0 30 day 6 months o Death, MI, or Urgent Intervention p = 0.051 p = 0.007 p < 0.001 p < 0.001 Reduction vs Stent Only Reduction vs Stent Only Abciximab + Stent 51% 47% Abciximab + Stent 51% 47% Abciximab Only 37% 24% Abciximab Only 37% 24%
World Wide Effect of Reopro if Used in All PTCA Procedures - Extrapolation from EPISTENT No. of Lives Saves: >2500 No. of MIs Prevented: >40,000 No. of emergency Revascularisation >6500 Prevented:
RESTORE Trial - Tirofiban for Patients with UA or acute MI undergoing PTCA 12 Placebo 24% Tirofibin 10.5 p=0.052 10 N = 2139 ) 8 8 Treatment was given for 36 hrs ) Baseline characteristics or risk ) stratification were not predictive 6 of treatment effect Composite Endpoint % (Death, MI, Urgent R The differences in death and MI ) rates was maintained over 6 months but the rate of 4 revascularisation remained unchanged Subgroup angiography study of ) 2 600 pts should no effect on restenosis 0 Treatment Arms R = Revascularisation.
Overview of Randomised Trials of GP IIb/IIIa Inhibitors During Coronary Intervention
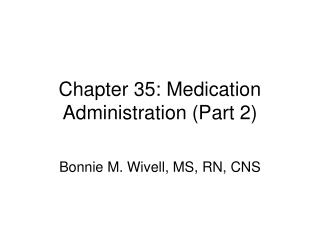
RAPPORT TRIAL - Reopro For Primary PTCA 35 N = 483 p= 0.038 0.02 48% 30 28.2 28.1 25 20 Placebo 16.6 Event Rate (%) Reopro 15 11.2 9.5 10 5.8 5 0 Endpoint A Endpoint B Bleeding Complications Endpoint A= Death, recurrent MI, urgent repeat TVR at 30 days. B= Death, recurrent MI, any repeat TVR (inc elective ones) at 6 month
GP IIb/IIIa Inhibitors for Coronary Intervention • In >15,000 patients GP IIb/IIIIa blockade shown to reduce risk of important acute ischaemic events by >50-60% during coronary intervention • The treatment effect extends to each of the components of the composite clinical endpoints (Death, MI, and emergency revascularisation) • The inhibition of ischaemic events is achieved early (12-48 hrs) and maintained up to 3 yrs
GP IIb/IIIa Inhibitors for Coronary Intervention • All patients regardless of their demographics, clinical, angiograhic, or procedural characteristic benefit • Patients with UAP and Diabetics obtain the greatest benefit • There may be heterogeneity among the different IIb/IIIa inhibitors. The greatest impact has been shown with Reopro. This may be due to its non-specific binding ability and its different pharmocokinetic profile
GP IIb/IIIa Inhibitors for Coronary Intervention • Reopro may be specially effective in reducing TVR and therefore restenosis in diabetes in association with coronary stenting but influence of GP IIb/IIIa inhibitors on restenosis in other groups remain unclear • Safety of these drugs is increased by keeping ACT ~200 during procedure and avoiding post-procedural heparin with early sheath removal • Economical aspects of this therapy needs to be evaluated
Who should have Reopro during Coronary Intervention • Patients with UAP at rest with ECG changes, or Refractory angina or Post MI angina particularly if: • Diabetic • Clot present • TIMI 3 flow not achieved • Troponin level is raised • ? In Rescue / Salvage PTCA