Download
1 / 1
10 likes | 111 Views
Family Involvement in Decisions for Older Adults with Dementia Sara Honn Qualls, Ph.D., University of Colorado at Colorado Springs. Study 2: Knowledge of Normal Aging Versus Dementia

E N D
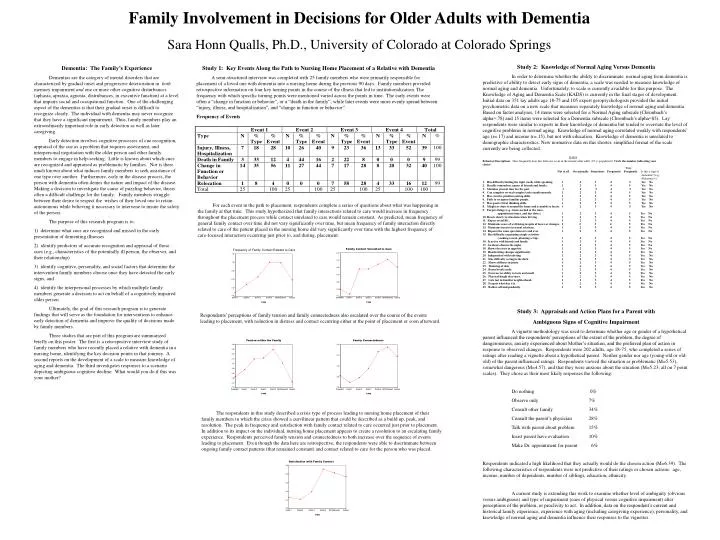
Family Involvement in Decisions for Older Adults with Dementia Sara Honn Qualls, Ph.D., University of Colorado at Colorado Springs Study 2: Knowledge of Normal Aging Versus Dementia In order to determine whether the ability to discriminate normal aging from dementia is predictive of ability to detect early signs of dementia, a scale was needed to measure knowledge of normal aging and dementia. Unfortunately, to scale is currently available for this purpose. The Knowledge of Aging and Dementia Scale (KADS) is currently in the final stages of development. Initial data on 351 lay adults age 18-75 and 105 expert geropsychologists provided the initial psychometric data on a new scale that measures separately knowledge of normal aging and dementia. Based on factor analyses, 14 items were selected for a Normal Aging subscale (Chronbach’s alpha=.78) and 15 items were selected for a Dementia subscale (Chronbach’s alpha=85). Lay respondents were similar to experts in their knowledge of dementia but tended to overstate the level of cognitive problems in normal aging. Knowledge of normal aging correlated weakly with respondents’ age (r=.17) and income (r=.15), but not with education. Knowledge of dementia is unrelated to demographic characteristics. New normative data on this shorter, simplified format of the scale currently are being collected. Study 3: Appraisals and Action Plans for a Parent with Ambiguous Signs of Cognitive Impairment A vignette methodology was used to determine whether age or gender of a hypothetical parent influenced the respondents’ perceptions of the extent of the problem, the degree of dangerousness, anxiety experienced about Mother’s situation, and the preferred plan of action in response to observed changes. Respondents were 202 adults, age 18-75, who completed a series of ratings after reading a vignette about a hypothetical parent. Neither gender nor age (young-old or old-old) of the parent influenced ratings. Respondents viewed the situation as problematic (M=5.53), somewhat dangerous (M=4.57), and that they were anxious about the situation (M=5.23; all on 7 point scales). They chose as their most likely responses the following: Do nothing 0% Observe only 7% Consult other family 34% Consult the parent’s physician 28% Talk with parent about problem 15% Insist parent have evaluation 10% Make Dr. appointment for parent 6% Respondents indicated a high likelihood that they actually would do the chosen action (M=6.39). The following characteristics of respondents were not predictive of their ratings or chosen actions: age, income, number of dependents, number of siblings, education, ethnicity. A current study is extending this work to examine whether level of ambiguity (obvious versus ambiguous) and type of impairment (cues of physical versus cognitive impairment) alter perceptions of the problem, or proclivity to act. In addition, data on the respondent’s current and historical family experience, experience with aging (including caregiving experience), personality, and knowledge of normal aging and dementia influence their responses to the vignettes. Dementia: The Family’s Experience Dementias are the category of mental disorders that are characterized by gradual onset and progressive deterioration in bothmemory impairment and one or more other cognitive disturbances (aphasia, apraxia, agnosia, distrubances, in executive function) at a level that impairs social and occupational function. One of the challenging aspect of the dementias is that their gradual onset is difficult to recognize clearly. The individual with dementia may never recognize that they have a significant impairment. Thus, family members play an extraordinarily important role in early detection as well as later caregiving. Early detection involves cognitive processes of cue recognition, appraisal of the cue as a problem that requires assessment, and interpersonal negotiation with the older person and other family members to engage in help-seeking. Little is known about which cues are recognized and appraised as problematic by families. Nor is there much known about what induces family members to seek assistance of one type over another. Furthermore, early in the disease process, the person with dementia often denies the nature and impact of the disease. Making a decision to investigate the cause of puzzling behavior, thusis often a difficult challenge for the family. Family members struggle between their desire to respect the wishes of their loved one to retain autonomous while believing it necessary to intervene to insure the safety of the person. The purpose of this research program is to: 1) determine what cues are recognized and missed in the early presentation of dementing illnesses 2) identify predictors of accurate recognition and appraisal of those cues (e.g., characteristics of the potentially ill person, the observer, and their relationship) 3) identify cognitive, personality, and social factors that determine the intervention family members choose once they have detected the early signs, and 4) identify the interpersonal processes by which multiple family members generate a decision to act on behalf of a cognitively impaired older person Ultimately, the goal of this research program is to generate findings that will serve as the foundation for interventions to enhance early detection of dementia and improve the quality of decisions made by family members. Three studies that are part of this program are summarized briefly on this poster. The first is a retrospective interview study of family members who have recently placed a relative with dementia in a nursing home, identifying the key decision points in that journey. A second reports on the development of a scale to measure knowledge of aging and dementia. The third investigates responses to a scenario depicting ambiguous cognitive decline: What would you do if this was your mother? Study 1: Key Events Along the Path to Nursing Home Placement of a Relative with Dementia A semi-structured interview was completed with 25 family members who were primarily responsible for placement of a loved one with dementia into a nursing home during the previous 90 days. Family members provided retrospective information on four key turning points in the course of the illness that led to institutionalization. The frequency with which specific turning points were mentioned varied across the points in time. The early events were often a “change in function or behavior”, or a “death in the family”, while later events were more evenly spread between “injury, illness, and hospitalization”, and “change in function or behavior”. Frequency of Events KADS Behavior Descriptions How frequently does this behavior occur in the normal older adult (65 +) population? Circle the number indicating your choice: Very Not at all Occasionally Sometimes Frequently Frequently Is this a sign of dementia? (e.g., Alzheimer’s) 1. Has difficulty finding the right words while speaking. 1 2 3 4 5 Yes No 2. Readily remembers names of friends and family. 1 2 3 4 5 Yes No 3. Mistakes present time for the past. 1 2 3 4 5 Yes No 4. Can complete several complex tasks simultaneously. 1 2 3 4 5 Yes No 5. Has creative problem solving skills. 1 2 3 4 5 Yes No 6. Fails to recognize familiar people. 1 2 3 4 5 Yes No 7. Has good critical thinking skills. 1 2 3 4 5 Yes No 8. Misplaces objects around the home and is unable to locate. 1 2 3 4 5 Yes No 9. Forgets things (e.g., items needed at the store, appointment times, and due dates). 1 2 3 4 5 Yes No 10. Reacts slowly to situations when driving. 1 2 3 4 5 Yes No 11. Enjoys social life. 1 2 3 4 5 Yes No 12. Maintains sense of well-being in spite of losses or changes. 1 2 3 4 5 Yes No 13. Maintains interest in sexual relations. 1 2 3 4 5 Yes No 14. Repeats the same question over and over. 1 2 3 4 5 Yes No 15. Has difficulty organizing simple activities (cooking a meal, planning a trip). 1 2 3 4 5 Yes No 16. Is active with friends and family. 1 2 3 4 5 Yes No 17. Awakens often in the night. 1 2 3 4 5 Yes No 18. Shows decrease in appetite. 1 2 3 4 5 Yes No 19. Handwriting changes significantly. 1 2 3 4 5 Yes No 20. Independent with toileting. 1 2 3 4 5 Yes No 21. Has difficulty seeing in the dark. 1 2 3 4 5 Yes No 22. Shows stiffness in joints. 1 2 3 4 5 Yes No 23. Thinning of skin. 1 2 3 4 5 Yes No 24. Bones break easily. 1 2 3 4 5 Yes No 25. Decrease in ability to taste and smell. 1 2 3 4 5 Yes No 26. Physical height decreases. 1 2 3 4 5 Yes No 27. Gets lost in familiar neighborhood. 1 2 3 4 5 Yes No 28. Forgets what day it is. 1 2 3 4 5 Yes No 29. Bathes self independently. 1 2 3 4 5 Yes No For each event in the path to placement, respondents complete a series of questions about what was happening in the family at that time. This study hypothesized that family interactions related to care would increase in frequency throughout the placement process while contact unrelated to care would remain constant. As predicted, mean frequency of general family contact over time did not vary significantly over time, but mean frequency of family interaction directly related to care of the patient placed in the nursing home did vary significantly over time with the highest frequency of care-focused interaction occurring just prior to, and during, placement. Respondents’ perceptions of family tension and family connectedness also escalated over the course of the events leading to placement, with reduction in distress and contact occurring either at the point of placement or soon afterward. The respondents in this study described a crisis type of process leading to nursing home placement of their family members in which the crisis showed a curvilinear pattern that could be described as a build up, peak, and resolution. The peak in frequency and satisfaction with family contact related to care occurred just prior to placement. In addition to its impact on the individual, nursing home placement appears to create a resolution to an escalating family experience. Respondents perceived family tension and connectedness to both increase over the sequence of events leading to placement. Even though the data here are retrospective, the respondents were able to discriminate between ongoing family contact patterns (that remained constant) and contact related to care for the person who was placed.