Download
1 / 34
340 likes | 433 Views
Innate Immunity: The First Line Against Infections. Juan Pablo Horcajada. Unidad de Enfermedades Infecciosas Hospital Universitario Marqués de Valdecilla Santander. Spain. Relevance. In adults there are important differences in susceptibility to infections

E N D
Innate Immunity: The First Line Against Infections Juan Pablo Horcajada. Unidad de Enfermedades Infecciosas Hospital Universitario Marqués de Valdecilla Santander. Spain.
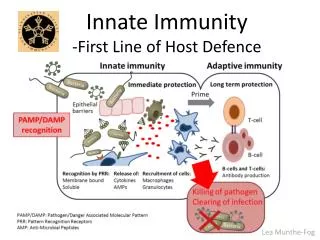
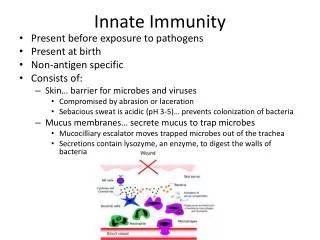
Relevance • In adults there are important differences in • susceptibility to infections • outcome of infections under treatment • Innate immune system is the “third column” of the immun system • There are new therapeutical possibilities
Innate immunity Cellular Immunity Humoral Inmunity
Index • The innate immune system • Mannose-binding lectin • MBL deficiency and infections: susceptibility and severity • Special populations: • Bone marrow transplant patients • HIV-infected patients
Humoral response Cellular response Antibodies Lymphocytes Immunity Innate Adaptative Non-specific Does not generate memory Specific Generates memory Humoral factors Cells External barriers Complement Acute phase proteins Neutrophils Monocytes NK Cells
CLASSIC PATHWAY Ag-Ab Complexes THE COMPLEMENT SYSTEM MBL PATHWAY Microbial surfaces ALTERNATIVE PATHWAY Microbial surfaces MBL-MASP2 MBL-MASP1 C3b C1q C1r C1s C4 C2 C3 C4b C2a C3a, C5a C3b C5b-C9 Inflamation, fagocyte recruitment Membrane attack complex, pathogen lysis Opsonization, elimination of immunocomplexes
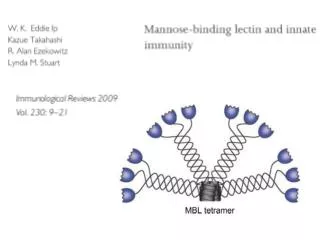
MBL TETRAMER Disulfur bond Proteases (masp) N-terminal Activation C’ collagen first region collagen second region DRC hexose Bacterial surface
Structure of MBL polipeptidic chain D Carbohidrate Recognition Domain (CRD) C Alpha helix region. Interacts with CRD and determines its spatial orientation Collagen region. Functions: fagocytosis, opsonization and protease binding for complement activation B Terminal NH2 segment. Oligomerization through N-terminal cisteins by disulfur bonds A
MBL gen polymorphisms Promotor Exon 1
Serum MBL levels related with different haplotipes High (>1000 ng/ml) HYPA LYQA LYPA Homozygous Sufficient Medium (500-1000 ng/ml) HYPA LYQA LYPA LXPA Heterozygous sufficient Low (200-500 ng/ml) HYPD LYQC LYPB HYPA LYQA LYPA Heterozygous Sufficient-insufficient Very Low (<200 ng/ml) HYPD LYPB LYQC LXPA Homozygous insufficient
MBL levels in relation with haplotypes Homozygous defficient
MBL binding to different microorganisms +++ Candida Aspergillus S. aureus S. pyogenes Bifidobacterium Veillonella ++ E. coli Klebsiella Haemophilus influenza B + S. agalactiae S. pneumoniae S. epidermidis Pseudomonas Enterococcus Clostridium Bacterioides
MBL defficiency and susceptibility to bacterial infections Meningococcal Infection Frequency of homozigous MBL-variants alleles in hospitalized patients 7,7% vs. 1,5% in non-infectious controls OR 6,5 p = 0.0006 Frequency in general population: 8,3% vs. 2,3% in healthy controls OR 4,5 p = 0.06 Hibberd ML. Lancet 1999;353:1049
MBL defficiency and susceptibility to bacterial infections Pneumococal infection Defficient homozygous Controls OR p 28/229 (12%) 18/353 (5%) 2,59 0.002 11/108 (10%) 36/679 (5%) --- 0.046 Roy S. Lancet. 2002;360:1176.
MBL levels in elective abdominal surgery and incidence of bacterial infections N=172 patients N infections: 10 (0,58%) M. Siassi. Biochem Soc Tras 2003;31:774
MBL defficiency associated with recurrent bacterial infections Gomi K. Chest 2004; 126:95–99
MBL defficiency and susceptibility to fungal infections Recurrent vaginal candidiasis Babula CID 2003 Sep 1;37(5):733
MBL defficiency and susceptibility to fungal infections Chronic necrotizing pulmonary Aspergillosis Defficients Haplotypes In Controls p in CNPA 7/10 (70%) 20/82 (25%) 0,004 Crosdale JID 2001
Bacteraemic Pyelonephritis N = 27 Non Bacteraemic Pyelonephritis N = 35 MBL defficiency and severity of infections Low MBL (n=13) 9 (33.3) 4 (11.4) Normal MBL (n=49) 18 (67.6) 31 (88.6) P=0.0362 test Smithson A. 2005 ECCMID . P-1824
Pyelonephritis with septic shock N = 7 Pyelonephritis without septic shock N = 55 MBL defficiency and severity of infections Low MBL (n=13) 4 (57) 9 (16.3) Normal MBL (n=49) 3 (43) 46 (83.7) P=0.030 Fisher exact test Smithson A. 2005 ECCMID . P-1824
Innate immunity Cellular Immunity Humoral Inmunity
MBL Serum levels and Susceptibility to opportunistic Infections in bone marrow transplant patients Prospective study (feb-oct 2005) BMT and infections Follow-up 6 months Periodic MBL serum levels determinations • RESULTS • 12 (50%) autologous and 12 (50%) alogenic. • 55% of infectious episodes: during neutropenic period. • 63% bacterial; 26% viral, 9% fungal • 6 (25%) died because an infectious complication
MBL<1000 * infeccion viral Crosstabulation Count infeccion viral n0 si Total MBL<1000 no 4 6 10 si 10 8 2 Total 12 8 20 P = 0,16 MBL<1000 *gram positive inf Crosstabulation Count gram positive infection no yes Total MBL<1000 no 8 3 11 si 7 2 9 P = 1 Total 15 5 20 MBL<1000 * gram negative infec Crosstabulation Count gram negative infection no yes Total MBL<1000 no 4 7 11 si 3 6 9 P = 1 Total 7 13 20 P = 0.16
MBL<1000 fungal infection no/yes Crosstabulation Count fungal infection no/yes no yes Total MBL<1000 no 11 11 si 6 3 9 P = 0,07 Total 17 3 20 Maximum MBL serum levels ng/mL • Confirmed fungal infection • -Pulmonary Aspergilosis • Pulmonary Mucormicosis • Systemic Candidiasis
Polymorphisms of the Mannose-Binding Lectin Gen and Susceptibility to Opportunistic Infections in HIV-Infected Patients A/A or A/0 n=151 460 (304) 48831 (154112) 0/0 n=39 527 (252) 36579 (152237) p 0.21 0.66 Genotypes CD4 count, mean (SD) Viral load, mean (SD) JP Horcajada et al. ICAAC 2004
S. pneumoniae p 0.65 1 0.28 A/A or A/0 n=151 32 (21) 5 (3.3) 17 (11) 0/0 n=39 7 (18) 1 (2.5) 7 (18) Genotypes Pneumococcal bacteremia Recurrent pneumococcal bacteremia Recurrent pneumonia JP Horcajada et al. ICAAC 2004
Candidiasis p 1 1 1 0.96 A/A or A/0 n=151 7 (4.6) 18 (12) 4 (2.6) 29 (19.2) 0/0 n=39 1 (2.5) 5 (13) 1 (2.5) 7 (18) Genotypes Oral (Muget), n(%) Esophageal, n(%) Vaginal, n(%) Any candidiasis, n(%) JP Horcajada et al. ICAAC 2004
Virus p 0.20 0.15 0.03 0.50 0.58 A/A or A/0 n=151 7 (4.6) 32 (21) 5 (3.3) 2 (1.3) 4 (2.6) 0/0 n=39 1 (2.5) 4 (10.2) 5 (13) 1 (2.5) 0 Genotypes Cytomegalovirus Herpes Zoster Recurrent Herpes simplex Progressive multifocal leukencephalopathy Molluscum contagiosum JP Horcajada et al. ICAAC 2004
Other OI p 1 0.52 0.50 0.10 0.73 1 A/A or A/0 n=151 6 (3.9) 10 (6.6) 2 (1.3) 3 (1.9) 13 (8.6) 1 (0.6) 0/0 n=39 1 (2.5) 3 (7.7) 1 (2.5) 3 (7.7) 2 (5.1) 0 Genotypes Toxoplasmosis Pneumocystis carinii MAI Hairy leukoplakia Condiloma Non-TB Mycobacteria JP Horcajada et al. ICAAC 2004
Tuberculosis p 0.20 1 1 0.35 0.048 A/A or A/0 n=151 15 (10) 3 (1.9) 1 (0.6) 8 (5.3) 27 (18) 0/0 n=39 1 (2.5) 1 (2.5) 0 0 2 (5.1) Genotypes Pulmonary, n(%) Lymph node, n(%) Bone, n(%) Milliary, n(%) Any TB, n(%) JP Horcajada et al. ICAAC 2004
Conclusions (I) • MBL is a key protein of the innate immune system • MBL serum level is genetically determined • Genetic polymorphisms are very prevalent • There is a higher predisposition for some infections in MBL-deficient patients
Conclusions (II) • MBL defficiency is associated with higher severity of infections • In bone marrow transplant MBL deficiency is associated with a higher incidence of invasive fungal infections. • No relation between low MBL levels and the incindence bacterial / viral infections and in these patients
Conclusions (III) • In HIV-infected patients MBL deficiency is associated with a higher incidence of recurrent herpes. On the contrary, tuberculosis is more frequent in patients With normal or high MBL levels. • Milliary tuberculosis is not detected in MBL-deficient HIV-infected patients.