Download
1 / 1
10 likes | 169 Views
Soluble tissue factor in Primary HIV Infection. Elizabeth Hamlyn 1,2 , Kiran Parmar 3 , Stephen Hickling 4 , John Frater 4 , Rodney Phillips 4 , Myra McClure 1 , Sarah Fidler 1 , and Beverley J Hunt 3 for the SPARTAC Investigators

E N D
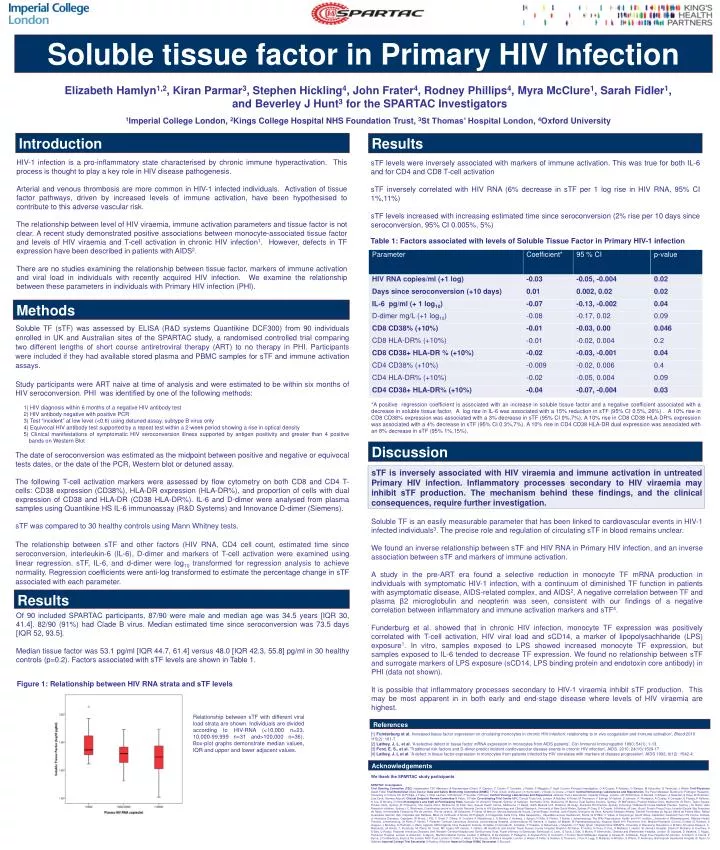
Soluble tissue factor in Primary HIV Infection Elizabeth Hamlyn1,2, Kiran Parmar3, Stephen Hickling4, John Frater4, Rodney Phillips4, Myra McClure1, Sarah Fidler1, and Beverley J Hunt3 for the SPARTAC Investigators 1Imperial College London, 2Kings College Hospital NHS Foundation Trust, 3St Thomas’ Hospital London, 4Oxford University Introduction Results HIV-1 infection is a pro-inflammatory state characterised by chronic immune hyperactivation. This process is thought to play a key role in HIV disease pathogenesis. Arterial and venous thrombosis are more common in HIV-1 infected individuals. Activation of tissue factor pathways, driven by increased levels of immune activation, have been hypothesised to contribute to this adverse vascular risk. The relationship between level of HIV viraemia, immune activation parameters and tissue factor is not clear. A recent study demonstrated positive associations between monocyte-associated tissue factor and levels of HIV viraemia and T-cell activation in chronic HIV infection1. However, defects in TF expression have been described in patients with AIDS2. There are no studies examining the relationship between tissue factor, markers of immune activation and viral load in individuals with recently acquired HIV infection. We examine the relationship between these parameters in individuals with Primary HIV infection (PHI). sTF levels were inversely associated with markers of immune activation. This was true for both IL-6 and for CD4 and CD8 T-cell activation sTF inversely correlated with HIV RNA (6% decrease in sTF per 1 log rise in HIV RNA, 95% CI 1%,11%) sTF levels increased with increasing estimated time since seroconversion (2% rise per 10 days since seroconversion, 95% CI 0.005%, 5%) Table 1: Factors associated with levels of Soluble Tissue Factor in Primary HIV-1 infection Methods • Soluble TF (sTF) was assessed by ELISA (R&D systems Quantikine DCF300) from 90 individuals enrolled in UK and Australian sites of the SPARTAC study, a randomised controlled trial comparing two different lengths of short course antiretroviral therapy (ART) to no therapy in PHI. Participants were included if they had available stored plasma and PBMC samples for sTF and immune activation assays. • Study participants were ART naive at time of analysis and were estimated to be within six months of HIV seroconversion. PHI was identified by one of the following methods: 1) HIV diagnosis within 6 months of a negative HIV antibody test 2) HIV antibody negative with positive PCR 3) Test “incident” at low level (<0.6) using detuned assay, subtype B virus only 4) Equivocal HIV antibody test supported by a repeat test within a 2-week period showing a rise in optical density 5) Clinical manifestations of symptomatic HIV seroconversion illness supported by antigen positivity and greater than 4 positive bands on Western Blot • The date of seroconversion was estimated as the midpoint between positive and negative or equivocal tests dates, or the date of the PCR, Western blot or detuned assay. • The following T-cell activation markers were assessed by flow cytometry on both CD8 and CD4 T-cells: CD38 expression (CD38%), HLA-DR expression (HLA-DR%), and proportion of cells with dual expression of CD38 and HLA-DR (CD38 HLA-DR%). IL-6 and D-dimer were analysed from plasma samples using Quantikine HS IL-6 immunoassay (R&D Systems) and Innovance D-dimer (Siemens). • sTF was compared to 30 healthy controls using Mann Whitney tests. • The relationship between sTF and other factors (HIV RNA, CD4 cell count, estimated time since seroconversion, interleukin-6 (IL-6), D-dimer and markers of T-cell activation were examined using linear regression. sTF, IL-6, and d-dimer were log10 transformed for regression analysis to achieve normality. Regression coefficients were anti-log transformed to estimate the percentage change in sTF associated with each parameter. *A positive regression coefficient is associated with an increase in soluble tissue factor and a negative coefficient associated with a decrease in soluble tissue factor. A log rise in IL-6 was associated with a 15% reduction in sTF (95% CI 0.5%, 26%) . A 10% rise in CD8 CD38% expression was associated with a 3% decrease in sTF (95% CI 0%,7%). A 10% rise in CD8 CD38 HLA-DR% expression was associated with a 4% decrease in sTF (95% CI 0.3%,7%). A 10% rise in CD4 CD38 HLA-DR dual expression was associated with an 8% decrease in sTF (95% 1%,15%). Discussion sTF is inversely associated with HIV viraemia and immune activation in untreated Primary HIV infection. Inflammatory processes secondary to HIV viraemia may inhibit sTF production. The mechanism behind these findings, and the clinical consequences, require further investigation. Soluble TF is an easily measurable parameter that has been linked to cardiovascular events in HIV-1 infected individuals3. The precise role and regulation of circulating sTF in blood remains unclear. We found an inverse relationship between sTF and HIV RNA in Primary HIV infection, and an inverse association between sTF and markers of immune activation. A study in the pre-ART era found a selective reduction in monocyte TF mRNA production in individuals with symptomatic HIV-1 infection, with a continuum of diminished TF function in patients with asymptomatic disease, AIDS-related complex, and AIDS2. A negative correlation between TF and plasma β2 microglobulin and neopterin was seen, consistent with our findings of a negative correlation between inflammatory and immune activation markers and sTF4. Funderburg et al. showed that in chronic HIV infection, monocyte TF expression was positively correlated with T-cell activation, HIV viral load and sCD14, a marker of lipopolysachharide (LPS) exposure1. In vitro, samples exposed to LPS showed increased monocyte TF expression, but samples exposed to IL-6 tended to decrease TF expression. We found no relationship between sTF and surrogate markers of LPS exposure (sCD14, LPS binding protein and endotoxin core antibody) in PHI (data not shown). It is possible that inflammatory processes secondary to HIV-1 viraemia inhibit sTF production. This may be most apparent in in both early and end-stage disease where levels of HIV viraemia are highest. Results Of 90 included SPARTAC participants, 87/90 were male and median age was 34.5 years [IQR 30, 41.4]. 82/90 (91%) had Clade B virus. Median estimated time since seroconversion was 73.5 days [IQR 52, 93.5]. Median tissue factor was 53.1 pg/ml [IQR 44.7, 61.4] versus 48.0 [IQR 42.3, 55.8] pg/ml in 30 healthy controls (p=0.2). Factors associated with sTF levels are shown in Table 1. Figure 1: Relationship between HIV RNA strata and sTF levels Relationship between sTF with different viral load strata are shown. Individuals are divided according to HIV-RNA (<10,000 n=23, 10,000-99,999 n=31 and>100,000 n=36). Box-plot graphs demonstrate median values, IQR and upper and lower adjacent values. References [1] Funderburg et al. Increased tissue factor expression on circulating monocytes in chronic HIV infection: relationship to in vivo coagulation and immune activation', Blood 2010 115(2): 161-7. [2] Lathey, J. L. et al. 'A selective defect in tissue factor mRNA expression in monocytes from AIDS patients', Clin Immunol Immunopathol 1990; 54(1): 1-13. [3] Ford, E. S., et al. 'Traditional risk factors and D-dimer predict incident cardiovascular disease events in chronic HIV infection', AIDS. 2010; 24(10):1509-17. [4] Lathey, J. L et al. 'A defect in tissue factor expression in monocytes from patients infected by HIV correlates with markers of disease progression', AIDS1992;6(12): 1542-4. Acknowledgements We thank the SPARTAC study participants SPARTAC Investigators Trial Steering Committee (TSC) Independent TSC Members: A Breckenridge (Chair), P Clayden, C Conlon, F Conradie, J Kaldor, F Maggiolo; F Ssali Country Principal Investigators: D A Cooper, P Kaleebu, G Ramjee, M Schechter, G Tambussi, J Weber Trial Physician Sarah Fidler Trial Statistician Abdel Babiker Data and Safety Monitoring Committee (DSMC) T Peto (Chair) A McLaren (in memoriam), V Beral, G Chene, J Hakim Central Immunology Laboratories and Repositories The Peter Medawar Building for Pathogen Research, University of Oxford, UK (R Phillips, J Frater, L Ohm Laursen, N Robinson, P Goulder, H Brown) Central Virology Laboratories and Repositories Jefferiss Trust Laboratories, Imperial College, London, UK (M McClure, D Bonsall, O Erlwein, A Helander, S Kaye, M Robinson, Lisa Cook, Gemma Adcock) Clinical Endpoint Review Committee N Paton, S Fidler Co-ordinating Trial Centre MRC Clinical Trials Unit, London (A Babiker, K Porter, M Thomason, F Ewings, M Gabriel, D Johnson, K Thompson, A Cursley, K Donegan, E Fossey, P Kelleher, K Lee, B Murphy, D Nock)Investigators and Staff at Participating Sites Australia: St Vincent’s Hospital, Sydney (A Kelleher), Northside Clinic, Melbourne (R Moore), East Sydney Doctors, Sydney, (R McFarlane), Prahran Market Clinic, Melbourne (N Roth), Taylor Square Private Clinic, Sydney (R Finlayson), The Centre Clinic, Melbourne (B Kiem Tee), Sexual Health Centre, Melbourne (T Read), AIDS Medical Unit, Brisbane (M Kelly), Burwood Rd Practice, Sydney (N.Doong) Holdsworth House Medical Practice, Sydney ( M. Bloch) Aids Research Initiative, Sydney ( C. Workman).Coordinating centre in Australia: National Centre in HIV Epidemiology and Clinical Research, University of New South Wales, Sydney (P Grey, D A Cooper, A Kelleher, M Law). Brazil: Projeto Praça Onze, Hospital Escola São Francisco de Assis, Universidade Federal do Rio de Janeiro, Rio de Janeiro. (M Schechter, P Gama, M Mercon, Monica Barbosa de Souza, Carina Beppu Yoshida, José Roberto Grangeiro da Silva, Adryane Sampaio Amaral, Daniele Fernandes de Aguiar, Maria de Fátima Melo, Rafael Quaresma Garrido) Italy: Ospedale San Raffaele, Milan (G Tambussi, S Nozza, M Pogliaghi, S ChiappettaL Della Torre, Elisa Gasparotto,), Ospedale Lazzaro Spallanzani, Roma (G D’Offizi, C Vlassi, A Corpolongo) South Africa: Capetown: Desmond Tutu HIV Centre, Institute of Infectious Diseases, Capetown (R Wood, J Pitt, C Orrell, F Cilliers, R Croxford, K Middelkoop, L G Bekker, C Heiberg, J Aploon, N Killa, E Fielder, T Buhler ) Johannesburg: The Wits Reproductive Health and HIV Institute, University of Witswatersrand, Hillbrow Health Precinct, Johannesburg. (H Rees, F Venter, T Palanee) Contract Laboratory Services, Johannesburg Hospital, Johannesburg (W Stevens, C Ingram, M Majam, M Papathanasopoulos) Kwazulu-Natal: HIV Prevention Unit, Medical Research Council, Durban (G Ramjee, S Gappoo, J Moodley, A Premrajh, L Zako) Uganda: MRC/Uganda Virus Research Institute, Entebbe (H Grosskurth, A Kamali, P Kaleebu, U Bahemuka, J Mugisha, H F Njaj) Spain: Hospital Clinic-IDIBAPS. University of Barcelona, Barcelona (J M Miro, M López-Dieguez, C. Manzardo, JA Arnaiz, T. Pumarola, M. Plana, M. Tuset, MC Ligero, MT García, T. Gallart, JM Gatell)UK and Ireland: Royal Sussex County Hospital, Brighton (M Fisher, K Hobbs, N Perry, D Pao, D Maitland, L Heald), St James’s Hospital, Dublin (F Mulcahy, G Courtney, S O’Dea, D Reidy), Regional Infectious Diseases Unit, Western General Hospital and Genitourinary Dept, Royal Infirmary of Edinburgh, Edinburgh (C Leen, G Scott, L Ellis, S Morris, P Simmonds), Chelsea and Westminster Hospital, London (B Gazzard, D Hawkins, C Higgs), Homerton Hospital, London (J Anderson, S Mguni), Mortimer Market Centre, London (I Williams, N De Esteban, P Pellegrino, A Arenas-Pinto, D Cornforth, J Turner) North Middlesex Hospital (J Ainsworth, A Waters), Royal Free Hospital (M Johnson, S Kinloch, A Carroll, P Byrne, Z Cuthbertson), Barts & the London NHS Trust, London (C Orkin, J Hand, C De Souza), St Mary’s Hospital, London (J Weber, S Fidler, E Hamlyn, E Thomson, J Fox, K Legg, S Mullaney, A Winston, S Wilson, P Ambrose), Birmingham Heartlands Hospital (S Taylor, G Gilleran) Imperial College Trial Secretariat S Keeling, A Becker Imperial College DSMC Secretariat C Boocock






