Download
1 / 2
20 likes | 395 Views
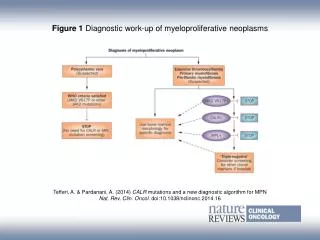
Establishing idiopathic intracranial hypertension. Associated or causative conditions. Aetiological diagnostic work up. Brain imaging. HISTORY .

E N D
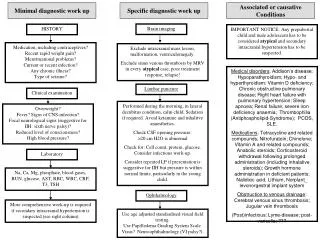
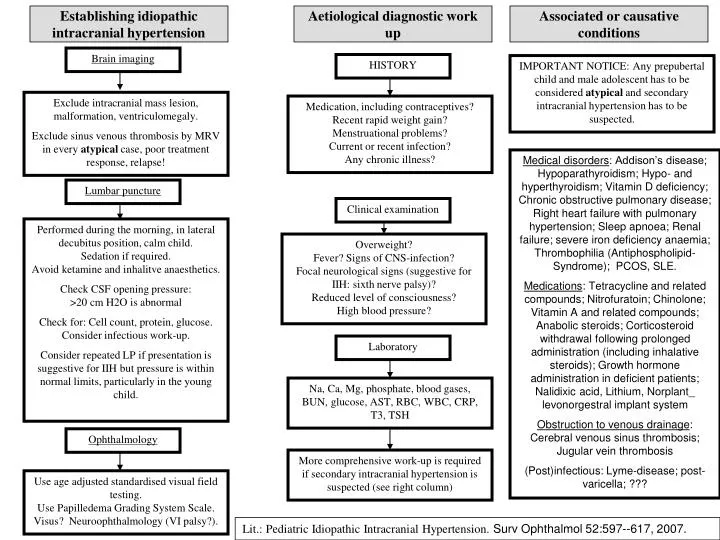
Establishing idiopathic intracranial hypertension Associated or causative conditions Aetiological diagnostic work up Brain imaging HISTORY IMPORTANT NOTICE: Any prepubertal child and male adolescent has to be considered atypical and secondary intracranial hypertension has to be suspected. Exclude intracranial mass lesion, malformation, ventriculomegaly. Exclude sinus venous thrombosis by MRV in every atypical case, poor treatment response, relapse! Medication, including contraceptives?Recent rapid weight gain?Menstruational problems?Current or recent infection?Any chronic illness? Medical disorders: Addison’s disease; Hypoparathyroidism; Hypo- and hyperthyroidism; Vitamin D deficiency; Chronic obstructive pulmonary disease; Right heart failure with pulmonary hypertension; Sleep apnoea; Renal failure; severe iron deficiency anaemia; Thrombophilia (Antiphospholipid-Syndrome); PCOS, SLE. Medications:Tetracycline and related compounds; Nitrofuratoin; Chinolone;Vitamin A and related compounds; Anabolic steroids; Corticosteroid withdrawal following prolonged administration (including inhalative steroids); Growth hormone administration in deficient patients; Nalidixic acid, Lithium, Norplant_ levonorgestral implant system Obstruction to venous drainage:Cerebral venous sinus thrombosis; Jugular vein thrombosis (Post)infectious: Lyme-disease; post-varicella; ??? Lumbar puncture Clinical examination Performed during the morning, in lateral decubitus position, calm child. Sedation if required. Avoid ketamine and inhalitve anaesthetics. Check CSF opening pressure: >20 cm H2O is abnormal Check for: Cell count, protein, glucose. Consider infectious work-up. Consider repeated LP if presentation is suggestive for IIH but pressure is within normal limits, particularly in the young child. Overweight? Fever? Signs of CNS-infection?Focal neurological signs (suggestive for IIH: sixth nerve palsy)? Reduced level of consciousness?High blood pressure? Laboratory Na, Ca, Mg, phosphate, blood gases, BUN, glucose, AST, RBC, WBC, CRP, T3, TSH Ophthalmology More comprehensive work-up is required if secondary intracranial hypertension is suspected (see right column) Use age adjusted standardised visual field testing.Use Papilledema Grading System Scale.Visus? Neuroophthalmology (VI palsy?). Lit.: Pediatric Idiopathic Intracranial Hypertension. Surv Ophthalmol 52:597--617, 2007.
Therapy of idiopathic intracranial hypertension Side effects: GI upset; paresthesias involving the lips, fingers, and toes; anorexia; electrolyte imbalance (metabolic acidosis). Kidney stones are rare, aplastic anemia exceedingly rare First choice Acetazolamid 15 (-100) mg/kg/day in 2 to 3 divided doses Regular ophthalmological follow-up. Check for: visual acuity, colour vision, visual field, papilledema Regular ophthalmological follow-up. Check for: visual acuity, colour vision, visual field, papilledema No response Not tolerated Replace by furosemide (0.3--0.6 mg/kg per day) No response Acetazolamid + furosemide OR consider topiramate (1,5-3 mg/kg/d) No response No response/progression No response/ progression Consider corticosteroids No response More comprehensive work-up is required as secondary intracranial hypertension is suspected. Contact neurosurgeon