Download
1 / 23
260 likes | 646 Views
Comparison of a Chromogenic Factor X Assay to International Normalized Ratio for Monitoring Oral Anticoagulation Therapy. David L. McGlasson; Major Benjamin G. Romick † , † , Bernard J. Rubal ‡ † Wilford Hall US Air Force Medical Center, Lackland Air Force Base, TX

E N D
Comparison of a Chromogenic Factor X Assay to International Normalized Ratio for Monitoring Oral Anticoagulation Therapy David L. McGlasson; Major Benjamin G. Romick†, †, Bernard J. Rubal‡ †Wilford Hall US Air Force Medical Center, Lackland Air Force Base, TX ‡ Brooke Army Medical Center, Fort Sam Houston, TX
Background • The International Normalized Ratio (INR) is the primary method for monitoring patients on oral anticoagulation therapy (OAT). • Numerous confounding variables limit monitoring of INR in patients on OAT • Lupus Anticoagulant (LA) • Converting direct thrombin inhibitors to OAT
Background • Chromogenic Assay for Factor X (CFX) has been validated for use in monitoring patients with LA who are on OAT • CFX is not affected by presence of LA and other variables that affect INR
Introduction • CFX has not been compared to INR in monitoring a broad population of patients on OAT • No universally defined range of values of CFX for: • Therapeutic anticoagulation • Supratherapeutic anticoagulation • Subtherapeutic anticoagulation
Introduction • Objectives of the present study: • Define the therapeutic range for CFX in this population • Assess the relationship between CFX and INR values in an outpatient “Coumadin Clinic” setting
Methods • INR and CFX levels were evaluated in randomly selected excess specimens from the coumadin clinic and normal subjects not receiving anticoagulant therapy • INR values were correlated to CFX for determining the following ranges for OAT patients: • Normal or Subtherapeutic INR < 2.0 • Therapeutic INR 2.0-3.0 • Supratherapeutic INR > 3.0
Methods • Instrumentation: • STA-R Evolution automated coagulation analyzer (Diagnostica-Stago, Inc.®, Parsippany, NJ) • Chromogenic Factor X assay (Diapharma, Inc.®, Westchester, OH) • INR performed with PT method using Neoplastine Cl+ with ISI of 1.28 and geometric mean of 13.8 seconds
Data Analysis • Overall correlation of INR to CFX assessed with inverse square method (Sigmaplot version 9.01; Systat Software, Inc, San Jose, Ca) • Goodness of fit expressed as the coefficient of determination: R2 • Receiver Operator Characteristic (ROC) curves used to discriminate therapeutic ranges (SPSS version 11.5, SPSS, Inc. Chicago, IL) • ROC area > 0.900 → highly discriminative • ROC area > 0.800 → good discrimination
Data Analysis • CFX ranges consistent with INR therapeutic ranges defined by plots of sensitivity and specificity versus CFX • Kolmogorov-Smirnov test employed to assess normality of CFX distributions among therapeutic subsets • Non-normally distributed data presented as median and 25th and 75th percentiles
Data Analysis • One-way Analysis of Variance on Ranks (Sigmastat version 3.11; Systat Software, Inc., San Jose, CA) used to assess differences in CFX among INR therapeutic ranges • Differences between groups assess used Dunn’s post hoc test • P values < 0.05 are considered significant
Results • 309 randomly selected OAT patients were tested • 30 normal subjects not on anticoagulants tested for comparison • Range of INR & CFX in OAT patients: • INR 0.92 – 12.76 • CFX 9 – 132%
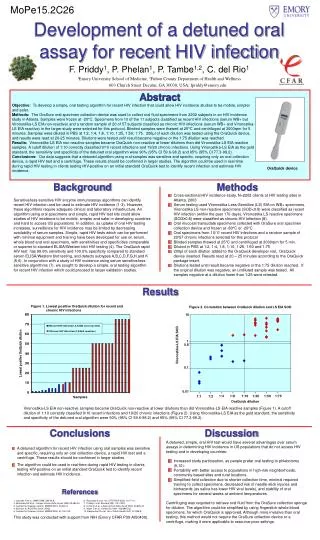
Figure 1. Good model fit between INR and CFX when expressed as a second order inverse function (N = 339, r2= 0.929; P<0.001). Open circles represent samples from normal control group (CFXn), closed circles represent patients receiving Coumadin therapy (CFXc).
Figure 2A. ROC curve using INR ≥ 2.0 as criteria for the threshold of therapeutic anticoagulation. Figure 2B (arrow) is a plot of sensitivity and specificity over the range of CFX values tested (N = 339). The arrow indicates the CFX value ≤ 35.5% that has maximum combined sensitivity and specificity for the INR therapeutic threshold (INR ≥ 2.0).
Figure 3A is a ROC curve for the patients with INR ≥ 2.0 (N = 240) using an INR value >3.0 for discriminating therapeutic form surpratherapeutic ranges of CFX. Figure 3B is a plot of sensitivityand specificity vs CFX values. Arrow indicates that CFX ≤ 23.5% is consistent with an INR >3.0.
Figure 4 depicts box plots (median: solid line, mean: dotted line, whiskers: 10th and 90th percentile) for CFX values categorized by INR therapeutic ranges. Significant differences were noted between all groups. Dashed lines indicate the CFX range (23.5%-35.5%) is equivalent to the INR therapeutic range (INR 2.0-3.0).
Conclusion • CFX correlates well with INR in a randomly selected group of OAT patients at varying levels of anticoagulation • R = 0.964 by inverse square function • CFX is highly discriminative for patients in therapeutic and subtherapeutic INR ranges • ROC curve area 0.948, p < 0.0001, n = 339 • CFX has good discrimination for patients in therapeutic and supratherapeutic INR range • ROC curve area 0.864, p < 0.0001, n = 240
Conclusion • CFX < 35.5% appears to be equivalent to INR > 2.0 • Sensitivity 91.7% • Specificity 91.9% • CFX < 23.5% suggests supratherapeutic anticoagulation equivalent to INR > 3.0 • Sensitivity 78.2% • Specificity 84.6%
Conclusion • Current findings suggest usefulness of CFX for monitoring oral anticoagulation in broad groups of patients seen in a coumadin clinic
Conclusion • Further study warranted to compare outcomes in OAT patients monitored with CFX and conventional INR methods • Bleeding events • Thromboembolism • Cost • Convenience • Availability
References • 1. Delate T, Witt DM, Jones JR, Bhardwaja B, Senser M. Falsely elevated international normalized • ratio values in patients undergoing anticoagulation therapy: a descriptive evaluation. Chest • 2007;131(3):816-822. • 2. Newman DH, Zhitomirsky I. The prevalence of nontherapeutic and dangerous international • normalized ratios among patients receiving warfarin in the emergency department. Ann Emerg • Med 2006;48(2):182-189. • 3. van den Besselaar AMHP, Hoekstra MMCL, Witteveen E, Didden JH, van der Meer FJM. • Influence of blood collection systems on the prothrombin time and international sensitivity index • determined with human and rabbit thromboplastin reagents. Am J Clin Pathol 2007;127(5):724- • 729. • 4. McGlasson DL. A comparison of INRs after local calibration of thromboplastin international • sensitivity indexes. Clin Lab Sci 2002;15(2):91-95. • 5. McGlasson DL. Laboratory variables that may affect test results in prothrombin times • (PT)/international sensitivity indexes. Clin Lab Sci 2003;34:124-128. • 6. McGlasson DL, Shaklee PN. A multi-instrument evaluation of a commercial chromogenic factor • X assay to monitor oral anticoagulation therapy. Blood 2004;104(11):4059. • 7. Shaklee PN, McGlasson DL. A multi-instrument evaluation of a chromogenic factor X assay for • monitoring oral anticoagulation therapy. Clin Chem 2005;51(Suppl 1):20112. • 8. Ortel TL, Moll S. Monitoring oral anticoagulant therapy in patients with lupus • anticoagulants.[comment]. Br J Haematol 1998;101(2):390-392.
References • 9. Robert A, Le Querrec A, Delahousse B, Caron C, Houbouyan L, Boutiere B, et al. Control of oral • anticoagulation in patients with the antiphospholipid syndrome--influence of the lupus • anticoagulant on International Normalized Ratio. Groupe Methodologie en Hemostase du Groupe • d'Etudes sur l'Hemostases et la Thrombose. Thromb Haemostasis 1998;80(1):99-103. • 10. Rosborough TK, Shepherd MF. Unreliability of international normalized ratio for monitoring • warfarin therapy in patients with lupus anticoagulant. Pharmacotherapy 2004; 24(7):838-842. • 11. Thom J, Ivey L, Gilmore G, Eikelboom JW. Evaluation of the phospholipid-rich dilute Russell's • viper venom assay to monitor oral anticoagulation in patients with lupus anticoagulant. Blood • Coagul Fibrinolysis 2004;15(4):353-357. • 12. Arpino PA, Demirjian Z, Van Cott EM. Use of the chromogenic factor X assay to predict the • international normalized ratio in patients transitioning from argatroban to warfarin. • Pharmacotherapy 2005;25(2):157-164. • 13. Perry SL, Samsa GP, Ortel TL. Point-of-care testing of the international normalized ratio in • patients with antiphospholipid antibodies. Thromb Haemostasis 2005: 94(6):1196-1202. • 14. Khamashta MA, Cuadrado MJ, Mujic F, Taub NA, Hunt BJ, Hughes GR. The management of • thrombosis in the antiphospholipid-antibody syndrome.[see comment]. N Engl J Med • 1995;332(15):993-997. • 15. Levine JS, Branch DW, Rauch J. The antiphospholipid syndrome.[see comment]. N Engl J • Med 2002;346(10):752-763. • 16. Sanfelippo MJ, Sennet J, McMahon EJ. Falsely elevated INRs in warfarin-treated patients with • the lupus anticoagulant. WMJ 2000 Jun;99(3):62-64. • 17. Trask AS, Gosselin RC, Diaz JA, Dager WE. Warfarin initiation and monitoring with clotting • factors II, VII, and X. Ann of Pharmacotherapy 2004 Feb;38:251-256.