Download
1 / 1
10 likes | 128 Views
Radiosurgery Alone or Postoperative Radiosurgery for 1-3 Brain Metastases. P.Madawala, MD 1 , R.Jin, MD 1 , J.Rock, MD 2 , B.Movsas, MD 1 , J.Kim, MD 1 , M.Rosenblum, MD 2 , Samuel Ryu, MD 1,2 Departments of Radiation Oncology 1 and Neurosurgery 2 ,

E N D
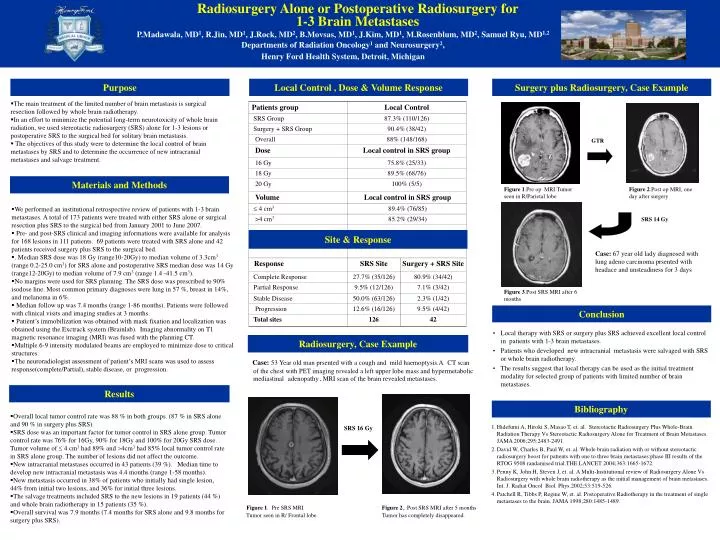
Radiosurgery Alone or Postoperative Radiosurgery for 1-3 Brain Metastases P.Madawala, MD1, R.Jin, MD1, J.Rock, MD2, B.Movsas, MD1, J.Kim, MD1, M.Rosenblum, MD2, Samuel Ryu, MD1,2 Departments of Radiation Oncology1 and Neurosurgery2, Henry Ford Health System, Detroit, Michigan Purpose Local Control , Dose & Volume Response Surgery plus Radiosurgery, Case Example • The main treatment of the limited number of brain metastasis is surgical resection followed by whole brain radiotherapy. • In an effort to minimize the potential long-term neurotoxicity of whole brain radiation, we used stereotactic radiosurgery (SRS) alone for 1-3 lesions or postoperative SRS to the surgical bed for solitary brain metastasis. • The objectives of this study were to determine the local control of brain metastases by SRS and to determine the occurrence of new intracranial metastases and salvage treatment. GTR Materials and Methods Figure 1.Pre op MRI.Tumor seen in R/Parietal lobe Figure 2.Post op MRI, one day after surgery • We performed an institutional retrospective review of patients with 1-3 brain metastases. A total of 173 patients were treated with either SRS alone or surgical resection plus SRS to the surgical bed from January 2001 to June 2007. • Pre- and post-SRS clinical and imaging informations were available for analysis for 168 lesions in 111 patients. 69 patients were treated with SRS alone and 42 patients received surgery plus SRS to the surgical bed. • . Median SRS dose was 18 Gy (range10-20Gy) to median volume of 3.3cm3 (range 0.2-25.0 cm3) for SRS alone and postoperative SRS median dose was 14 Gy (range12-20Gy) to median volume of 7.9 cm3 (range 1.4 -41.5 cm3). • No margins were used for SRS planning. The SRS dose was prescribed to 90% isodose line. Most common primary diagnoses were lung in 57 %, breast in 14%, and melanoma in 6%. • Median follow up was 7.4 months (range 1-86 months). Patients were followed with clinical visits and imaging studies at 3 months. • Patient’s immobilization was obtained with mask fixation and localization was obtained using the Exctrack system (Brainlab). Imaging abnormality on T1 magnetic resonance imaging (MRI) was fused with the planning CT. • Multiple 6-9 intensity modulated beams are employed to minimize dose to critical structures. • The neuroradiologist assessment of patient’s MRI scans was used to assess response(complete/Partial), stable disease, or progression. SRS 14 Gy Site & Response Case: 67 year old lady diagnosed with lung adeno carcinoma prsented with headace and unsteadiness for 3 days Figure 3.Post SRS MRI after 6 months Conclusion • Local therapy with SRS or surgery plus SRS achieved excellent local control in patients with 1-3 brain metastases. • Patients who developed new intracranial metastasis were salvaged with SRS or whole brain radiotherapy. • The results suggest that local therapy can be used as the initial treatment modality for selected group of patients with limited number of brain metastases. Radiosurgery, Case Example Case:53 Year old man prsented with a cough and mild haemoptysis.ACT scan of the chest with PET imaging revealed a left upper lobe mass and hypermetabolic mediastinaladenopathy.MRI scan of the brain revealed metastases. Results Bibliography • Overall local tumor control rate was 88 % in both groups. (87 % in SRS alone and 90 % in surgery plus SRS). • SRS dose was an important factor for tumor control in SRS alone group. Tumor control rate was 76% for 16Gy, 90% for 18Gy and 100% for 20Gy SRS dose. Tumor volume of 4 cm3 had 89% and 4cm3 had 85% local tumor control rate in SRS alone group. The number of lesions did not affect the outcome. • New intracranial metastases occurred in 43 patients (39 %). Median time to develop new intracranial metastasis was 4.4 months (range 1-58 months). • New metastasis occurred in 38% of patients who initially had single lesion, 44% from initial two lesions, and 36% for initial three lesions. • The salvage treatments included SRS to the new lesions in 19 patients (44 %) and whole brain radiotherapy in 15 patients (35 %). • Overall survival was 7.9 months (7.4 months for SRS alone and 9.8 months for surgery plus SRS). • Hidefumi A, Hiroki S, Masao T, et. al. Stereotactic Radiosurgery Plus Whole-Brain Radiation Therapy Vs Stereotactic Radiosurgery Alone for Treatment of Brain Metastases. JAMA 2006;295:2483-2491. • David W, Charles B, Paul W, et. al. Whole brain radiation with or without stereotactic radiosurgery boost for patients with one to three brain metastases:phase III results of the RTOG 9508 randamised trial.THE LANCET 2004;363:1665-1672. • Penny K, John H, Steven J, et. al. A Multi-Institutional review of Radiosurgery Alone Vs Radiosurgery with whole brain radiotherapy as the initial management of brain metastases. Int. J. Radiat Oncol Biol. Phys.2002;53:519-526. • Patchell R, Tibbs P, Regine W, et. al. Postoperative Radiotherapy in the treatment of single metastases to the brain. JAMA 1998;280:1485-1489. SRS 16 Gy Figure 1. Pre SRS MRIFigure 2,. Post SRS MRI after 5 months Tumor seen in R/ Frontal lobe. Tumor has completely disappeared.



















