Download
1 / 83
1.07k likes | 2.57k Views
Define Hormone. The term hormone is derived from a Greek verb meaning – to excite or arouse Hormone is a chemical messenger that is released in one tissue (endocrine tissue/gland) and transported in the bloodstream to reach specific cells in other tissues

E N D
Define Hormone • The term hormone is derived from a Greek verb meaning – to excite or arouse • Hormone is a chemical messenger that is released in one tissue (endocrine tissue/gland) and transported in the bloodstream to reach specific cells in other tissues • Regulate the metabolic function of other cells • Have lag times ranging from seconds to hours • Tend to have prolonged effects
Endocrine versus Nervous system • Both use chemical communication • Both are being regulated primarily by negative feedback • Released in synapse • Close to target cells • Signal to release by action potential • Short live effect • Crisis management Neurotransmitters Hormones • Released to bloodstream • Can be distant from target cells • Different types of signal • Long term effect • Ongoing processes
Control of Hormone Release • Blood levels of hormones: • Are controlled by negative feedback systems • Vary only within a narrow desirable range • Hormones are synthesized and released in response to: • Humoral stimuli • Neural stimuli • Hormonal stimuli
Humoral Stimuli • Secretion of hormones in direct response to changing blood levels of ions and nutrients • Example: concentration of calcium ions in the blood • Declining blood Ca2+ concentration stimulates the parathyroid glands to secrete PTH (parathyroid hormone) • PTH causes Ca2+ concentrations to rise and the stimulus is removed
Neural Stimuli • Neural stimuli – nerve fibers stimulate hormone release • Preganglionic sympathetic nervous system (SNS) fibers stimulate the adrenal medulla to secrete catecholamines Figure 16.5b
Hormonal Stimuli • Hormonal stimuli – release of hormones in response to hormones produced by other endocrine organs • The hypothalamic hormones stimulate the anterior pituitary • In turn, pituitary hormones stimulate targets to secrete still more hormones
Chemical structure AA derivatives Peptides lipids small proteins: GH,PRL • Tyrosine: • Thyroid hormones • Catecholamines (Epinephrine, norepinephrine • Tryptophan: • Dopamine, serotonin, melatonin Eicosanoid: prostaglandins Glycoproteins: TSH, LH, FSH short peptides: ADH, OT steroids
Distribution of Hormones in bloodstream • Freely circulating (most hormones) • Hormones that are freely circulating remain functional for less than one hour and some as little as 2 minutes • Freely circulating hormones are inactivated when: * bind to receptors on target cells * being broken down by cells of the liver or kidneys * being broken down by enzymes in the plasma or interstitial fluid • Bound to transport proteins – thyroid and steroid hormones (>1% circulate freely) • Remain in circulation longer
Hormones: Classification Table 7-1
Receptors for hormones are located: • on the cell membranes of target cells • In the cytoplasm or nucleus
Mechanisms of Hormone Action • Two mechanisms, depending on their chemical nature • Water-soluble hormones (all amino acid–based hormones except thyroid hormone) • Cannot enter the target cells • Act on plasma membrane receptors • Coupled by G proteins to intracellular second messengers that mediate the target cell’s response • Lipid-soluble hormones (steroid and thyroid hormones) • Act on intracellular receptors that directly activate genes
Receptors on the cell membrane • Hormones do not induces changes in cell activity directly but via the induction of the appearance and action of other agents • Hormones are referred to as first messengers and the agents that are activated by the hormones are called second messengers. • All amino-acid hormones (with exception of the thyroid hormone) exert their signals through a second messenger system: • cAMP • PIP
Amino Acid-Based Hormone Action: cAMP Second Messenger • Hormone (first messenger) binds to its receptor, which then binds to a G protein • The G protein is then activated • Activated G protein activates the effector enzyme adenylate cyclase • Adenylate cyclase generates cAMP (second messenger) from ATP • cAMP activates protein kinases, which then cause cellular effects
Hormone Protein receptor G protein (inactive) G protein activated Effects on cAMP Levels Many G proteins, once activated, exert their effects by changing the concentration of cyclic-AMP, which acts as the second messenger within the cell. Hormone Hormone Protein receptor Protein receptor G protein activated Increased production of cAMP G protein activated Enhanced breakdown of cAMP PDE adenylate cyclase Acts as second messenger kinase Reduced enzyme activity Opens ion channels Activates enzymes In some instances, G protein activation results in decreased levels of cAMP in the cytoplasm. This decrease has an inhibitory effect on the cell. If levels of cAMP increase, enzymes may be activated or ion channels may be opened, accelerating the metabolic activity of the cell. Examples: Examples: • Epinephrine and norepinephrine (β receptors) • Calcitonin • Parathyroid hormone • ADh, ACTH, FSH, LH, TSH • Glucagon • Epinephrine and norepineph- rine (α2 receptors)
Extracellular fluid 1 Hormone (1st messenger)binds receptor. Adenylate cyclase G protein (GS) 5 cAMP acti-vates proteinkinases. Receptor Activeproteinkinase GDP Inactiveprotein kinase 2 3 4 Receptoractivates Gprotein (GS). G proteinactivatesadenylatecyclase. Adenylatecyclaseconverts ATPto cAMP (2ndmessenger). Hormones thatact via cAMPmechanisms: Triggers responses oftarget cell (activatesenzymes, stimulatescellular secretion,opens ion channel,etc.) GlucagonPTHTSHCalcitonin EpinephrineACTHFSHLH Cytoplasm Figure 16.2, step 5
Amino Acid-Based Hormone Action: PIP-Calcium • Hormone binds to the receptor and activates G protein • G protein binds and activates phospholipase • Phospholipase splits the phospholipid PIP2 into diacylglycerol (DAG) and IP3 (both act as second messengers) • DAG activates protein kinases; IP3 triggers release of Ca2+ stores • Ca2+ (third messenger) alters cellular responses
Amino Acid-Based Hormone Action: PIP Mechanism Extracellular fluid Hormone DAG 1 4 5 Active protein kinase C 2 3 PIP2 GTP GTP Receptor Gq Inactive protein kinase C GDP GTP IP3 Phospholipase C Catecholamines TRH ADH GnRH Oxytocin Triggers responses of target cell 5 Endoplasmic reticulum 6 Cytoplasm Ca2+ Ca2+- calmodulin Figure 16.3
Hormone Protein receptor G protein (inactive) G protein activated Effects on Ca2+ Levels Some G proteins use Ca2+ as a second messenger. Hormone Protein receptor G protein activated PLC, DAG, and IP3 Opening of Ca2+ channels Release of stored Ca2+ from ER or SER Ca2+ acts as second messenger Calmodulin Activates enzymes Examples: • Epinephrine and norepinephrine (α1 receptors) • Oxytocin • Regulatory hormones of hypothalamus • Several eicosanoids
Steroid Hormones: Action 1 Most hydrophobic steroids are bound to plasma protein carriers. Only unbound hormones can diffuse into the target cell. Blood vessel Steroid hormone Cell surface receptor 2a Rapid responses 1 2 Steroid hormone receptors are in the cytoplasm or nucleus. 2 Protein carrier Nucleus 2a Some steroid hormones also bind to membrane receptors that use second messenger systems to create rapid cellular responses. Cytoplasmic receptor Nuclear receptor DNA Interstitial fluid 3 The receptor-hormone complex binds to DNA and activates or represses one or more genes. 3 Endoplasmic reticulum Transcription produces mRNA Cell membrane 4 Activated genes create new mRNA that moves back to the cytoplasm. 5 4 New proteins Translation 5 Translation produces new proteins for cell processes. Figure 7-7, steps 1–5
http://arbl.cvmbs.colostate.edu/hbooks/pathphys/endocrine/moaction/change.htmlhttp://arbl.cvmbs.colostate.edu/hbooks/pathphys/endocrine/moaction/change.html
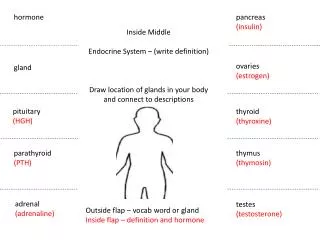
Pancreas structure Exocrine pancreas (99% of volume) Cells (pancreatic acini) forming glands and ducts that secrete pancreatic fluid and enzymes with digestive function Endocrine pancreas (1%) Small groups of cells scattered in clusters (pancreatic islets) that secrete hormones
How does the body control blood glucose levels Increased rate of glucose transport into target cell Increased rate of glucose utilization and ATP generation Increased conversion of glucose to glycogen Increased amino acid absorption and protein synthesis Beta cells secrete insulin. Increased triglyceride synthesis in adipose tissue HOMEOSTASIS RESTORED HOMEOSTASIS DISTURBED Blood glucose levels decrease Rising blood glucose levels Rising blood glucose levels HOMEOSTASIS Normal blood glucose levels (70-110 mg/dL) HOMEOSTASIS DISTURBED Falling blood glucose levels HOMEOSTASIS RESTORED Falling blood glucose level Blood glucose levels increase Alpha cells secrete glucagon Increased breakdown of glycogen to glucose (in liver, skeletal muscle) Increased breakdown of fat to fatty acids (in adipose tissue) Increased synthesis and release of glucose (in liver)
Endocrine Reflex Pathways: Insulin release KEY Blood glucose Eat a meal Stimulus Receptor Stretch receptor in digestive tract Efferent path Effector Tissue response Afferent neuron Sensory neuron CNS Efferent neuron Integrating center Negative feedback Efferent neuron Systemic response Pancreas Insulin Blood glucose Target tissues Glucose uptake and utilization Figure 7-9
Effects of Insulin Binding to its receptors • Insulin facilitates entry of glucose cells by binding to a membrane receptor • The complex insulin-receptor make a specific carrier protein (GLUT4) available • Once at the cell surface, GLUT4 facilitates the passive diffusion of circulating glucose down its concentration gradient into cells. • Receptors for insulin are present in most cell membranes (insulin-dependant cells) • Cells that lack insulin receptors are cells in the brain, kidneys, lining of the digestive tract and RBC (insulin-independent cells). • Those cells can absorb and utilize glucose without insulin stimulation.
Effects of Insulin • Acceleration of glucose uptake as a result from an increase of the number of glucose carrier proteins • Acceleration of glucose utilization and increased ATP production • Stimulation of glycogen formation in the liver and muscle cells • Inhibits glycogenolysis (break down of glycogen) and gluconeogenesis (glucose building) • Stimulation of amino acid absorption and protein synthesis • Stimulation of triglyceride formation in adipose tissue • As a result glucose concentration in the blood decreases
Glucagon • Released by alpha cells • A 29-amino-acid polypeptide hormone that is a potent hyperglycemic agent (what does it mean?) • it promotes: • Glycogenolysis – the breakdown of glycogen to glucose in the liver and skeletal muscle • Gluconeogenesis – synthesis of glucose from lactic acid and noncarbohydrates in the liver • Release of glucose to the blood from liver cells • breakdown of triglycerides in adipose tissue
Adrenal (Suprarenal) Glands • Structurally and functionally, they are two glands in one • Adrenal medulla – neural tissue; part of the sympathetic nervous system • Adrenal cortex - three layers of glandular tissue that synthesize and secrete corticosteroids
Adrenal Cortex • Synthesizes and releases steroid hormones called corticosteroids • Different corticosteroids are produced in each of the three layers • Zonaglomerulosa – glomerulus- little ball. Secretes mineralocorticoids – main one aldosterone • Zonafasciculata– glucocorticoids (chiefly cortisol) • Zonareticularis – gonadocorticoids (chiefly androgens) • Check point - Which of the layers will be part of glucose levels control?
Zonafasciculata - Glucocorticoids (Cortisol/hydrocortisone) • Main hormones secreted are the Cortisol/hydrocortisone and small amounts of corticosterone • It protects against hypoglycemia by stimulating catabolism of energy stores. • While adrenaline is responsible for rapid metabolic responses the glucocorticoids are responsible for long-term stress: • Glucocorticoids accelerate the rates of glucose synthesis and glycogen formation – especially in the liver • Adipose tissue responds by releasing fatty acids into the blood and the tissues start to utilize fatty acids as source of energy - glucose-sparing effect (GH has similar effect and will be discussed later) • Clucocorticoids also have anti-inflammatory effect – inhibit the activities of WBC (use?)
Pathway For the Control of Cortisol Secretion Circadianrhythm Stress Hypothalamus CRH long-loop negative feedback Anteriorpituitary ACTH Adrenalcortex Cortisol Immunesystem Adiposetissue Muscle Liver Functionsuppressed Gluco-neogenesis Proteincatabolism Lipolysis Figure 23-3
Diabetes Mellitus (DM) • Two types: • Type I results from the destruction of beta cells and the complete loss of insulin (hypoinsulinemia) • Type II is the most common type (90%) and is a result of decrease sensitivity of cells to insulin (insulin resistance). Type II is accompanied by hyperinsulinemia (what is that? Why?). • Type II is associated with excess weight gain and obesity but the mechanisms are unclear. • Other reasons that were associated with type II diabetes: pregnancy, polycystic ovary disease, mutations in insulin receptors and others
Type 1 and Type 2 Diabetes Mellitus Table 24.1
Diabetes Mellitus (DM) effects • Increase in blood glucose due to diabetes causes • Increase in glucose loss in urine • Dehydration of cells – since glucose does not diffuse through cell membrane and there is an increase in osmotic pressure in the extracellualr fluid. • In addition, the loss of glucose in the urine causes osmotic diuresis - decrease in water reabsorption in the kidney. • The result is • Polyuria – huge urine output and dehydration. • Polydipsia – excessive thirst
Diabetes Mellitus (DM) effects • Polyphagia – excessive hunger and food consumption because cells are starving • Damage to blood vessels and poor blood supply to different tissues • Increase use of lipids as a source of energy by the cells and increase release of keto bodies – ketosis and changes of blood pH (acidosis). That leads to increased respiratory rate
Hormones that control minerals and water • We will see the different glands that control: • Sodium – Adrenal gland • Which layer and what hormone group? • Calcium – Thyroid and parathyroid, kidney • Water - hypothalamus
Zonaglomerulosa – Mineralocorticoids • Aldosterone secretion is stimulated by: • Rising blood levels of K+ • Low blood Na+ • Decreasing blood volume or pressure
Zonaglomerulosa- Mineralocorticoids • The mineralocorticoids are steroids that affect the electrolytes composition of the body extracellular fluids. • Aldosterone – most important mineralocorticoid • Maintains Na+ balance by reducing excretion of sodium from the body • Stimulates re-absorption of Na+ by the kidneys • Prevents the loss of Na+ by the kidneys, sweat glands, salivary glands and digestive system • As a result of Na+ reabsorption there is also water reabsorption • The retention of Na+ is accompanied by a loss of K+
Protein hormones that control calcium • Parathyroid gland – PTH • PTH—most important hormone in Ca2+homeostasis • Thyroid gland – calcitonin • Liver and Kidney - Calcitriol – also known as vitamin D3
Calcium Balance in the Body • Total body calcium = intake output • Total body calcium is divided into three pools • Extracellular calcium (0.1% of total) • Intracellular calcium (0.9% of total) • Calcium in bone matrix (99% of total) • Ca2+ ions in the extracellular fluid move freely in and out of plasma • Extracellular fluid calcium is carefully regulated
Body Calcium is Carefully Regulated Small intestine Dietarycalcium Calciumin feces Ca2+ Calcitriol(PTH, prolactin) * Some calcium is secretedinto the small intestine. Bone ECF Kidney Passivefiltration Calcitonin Ca2+ inkidneytubules [Ca2+]2.5 mM Ca2+ PTH PTH CalcitriolCortisol Calcitonin Electrochemicalgradient Activetransport [free Ca2+]0.001 mM Ca2+in urine Cells KEY PTH = parathyroid hormone Figure 23-17
Simple Endocrine Reflex: Parathyroid Hormone Low plasma [Ca2+] Negative feedback Parathyroid cell Parathyroid hormone Bone and kidney Kidney reabsorption of calcium Production of calcitriol leads to intestinal absorption of Ca2+ Bone resorption Plasma [Ca2+] Figure 7-10
Effects of Parathyroid Hormone • PTH release increases Ca2+ in the blood: • Stimulates osteoclasts to digest bone matrix • Enhances the reabsorption of Ca2+ and the secretion of phosphate by the kidneys • Increases absorption of Ca2+ by intestinal mucosal • Rising Ca2+ in the blood inhibits PTH release (what type of control is it?) • The antagonist is the Calcitonin secreted by the thyroid gland
Calcitriol • Body makes calcitriol from vitamin D • Vitamin D can be ingested or produced in the skin • Calcitriol causes an increase in calcium absorption in the intestine • Calcitriol production in the kidneys is promoted by PTH
PTH Control of Calcium Balance Diet(fortified milk, fishoil, egg yolks) Endogenousprecursors Sunlighton skin Vitamin D Liver 25-hydroxycholecalciferol(25(OH)D3) Parathyroidhormone PlasmaCa2+ Kidney Calcitriol(1,25-dihydroxycholecalciferol) Bone,distal nephron, and intestine PlasmaCa2+ Figure 23-20
Calcitonin • A peptide hormone produced by the parafollicular, or C cells • Lowers blood calcium levels • Antagonist to parathyroid hormone (PTH)
Calcitonin • Calcitonin targets the skeleton, where it: • Inhibits osteoclast activity (and thus bone resorption) and release of calcium from the bone matrix • Stimulates calcium uptake and incorporation into the bone matrix • Regulated by a humoral (calcium ion concentration in the blood) negative feedback mechanism
Hormones that are involved in water balance • Anti diuretic hormone (ADH) – hypothalamus (stored in the neurohypophysis) • Aldosterone • Atrial natriuretic peptide (ANP) - heart