Download
1 / 66
660 likes | 723 Views
Life Cycle Nutrition: Pregnancy and Lactation. Chapter 15. Nutrition Prior to Pregnancy. Nutrition can affect fertility Preparation before pregnancy Achieve and maintain healthy body weight Choose an adequate and balanced diet Take a multivitamin for the folate (one of the DGA’s)

E N D
Nutrition Prior to Pregnancy • Nutrition can affect fertility • Preparation before pregnancy • Achieve and maintain healthy body weight • Choose an adequate and balanced diet • Take a multivitamin for the folate (one of the DGA’s) • Be physically active • Receive regular medical care • Manage chronic conditions • Avoid harmful influences (drugs, tobacco, excess alcohol)
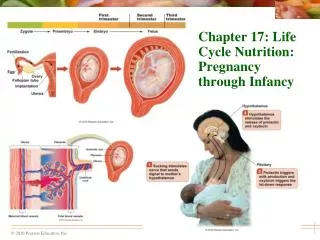
Growth and Development During Pregnancy • Placental development • Develops in uterus in the early days post-conception • Amniotic sac and umbilical cord • Expelled during childbirth • Interweaving of fetal and maternal blood vessels delivering O2 and nutrients and carrying out waste • Metabolically active organ: • Yes, it’s an organ • Requires energy and nutrients • Produces hormones that maintain pregnancy and prep for lactation
The arrows indicate the direction of blood flow. Umbilical cord Uterine wall Placenta Amniotic sac In the placenta, maternal blood vessels lie side by side with fetal blood vessels that reach the fetus through the umbilical cord.
Pool of mother's blood Fetal artery Fetal vein Fingerlike projections (called placental villi) contain fetal blood vessels and extend into the pool of mother’s blood. No actual mingling of fetal and maternal blood occurs, but substances pass back and forth. Umbilical cord Thus, oxygen and nutrients from the mother’s blood enter fetal vessels, and waste products are removed. Umbilical vein Umbilical arteries Mother’s veins carry fetal wastes away. Mother’s arteries bring fresh blood with oxygen and nutrients to the fetus. Fetal portion of placenta Maternal portion of placenta
Growth and Development During Pregnancy • Fetal growth and development • Fertilization of an ovum by a sperm • Zygote during 1st week • Rapid division to become blastocyst • Implantation in uterine wall • Embryo- 2-8 weeks • 1-1/4 inch at 8 weeks: has CNS, CVS, GI tract, fingers, toes • Fetus- 8-40 weeks • Full-term at 38-42 weeks, avg. 6.5-8 lbs
1) A newly fertilized ovum is about the size of a period at the end of this sentence. This zygote at less than one week after fertilization is not much bigger and is ready for implantation.
2) After implantation, the placenta develops and begins to provide nourishment to the developing embryo. An embryo 5 weeks after fertilization is about 1 / 2 inch long.
3)A fetus after 11 weeks of development is just over an inch long. Notice the umbilical cord and blood vessels connecting the fetus with the placenta.
4) A newborn infant after nine months of development measures close to 20 inches in length. From 8 weeks to term, this infant grew 20 times longer and 50 times heavier.
Growth and Development During Pregnancy • Critical periods • Times of intense development, rapid cell division • Critical periods occur early in pregnancy • Certain cellular activities can occur only during these times • Adverse influences on organ and tissue development • Each organ has its own critical period
An adverse influence felt late temporarily impairs development, but a full recovery is possible. Normal development An adverse influence felt early permanently impairs development, and a full recovery never occurs. Time Critical period
Growth and Development During Pregnancy • Neural tube defects – >300,000 births/yr worldwide • 1) Anacephaly • Brain either missing or fails to develop • 2) Spina bifida • Incomplete closure of spinal cord & its bony encasement • Varying degrees of paralysis → death • Clubfoot, dislocated hip, curved spine, retardation, motor /sensory loss • - Research on root causes: gene-gene, gene-nutrient, gene-environment • - Risk factors- family hx, maternal DM or obesity, anti-seizure meds, mutation in folate-related enzymes • -Folate supplementation 400 µg/d one month prior to conception and through 1st trimester • - Public health recommendation to “all women of childbearing age”
At 4 weeks, the neural tube has yet to close (notice the gap at the top). At 6 weeks, the neural tube (outlined by the delicate red vertebral arteries) has successfully closed.
Spina Bifida Spina Bifida Normal Spine Meninges Vertebra Spinal cord Spinal fluid Spina Bifida Spine Spine
Growth and Development During Pregnancy • Chronic diseases cont’d • Adverse influences at critical times during fetal development • Malnutrition – folate deficiency • Type 2 diabetes • Maternal inadequate nutrition affects cardiovascular growth during placental & gestational development → infant hypertension, lipid metabolism, immune system → adult health • Fetal programming • Mother’s nutrition during pregnancy may change gene expression in fetus, influence disease susceptibility later in life
Maternal Weight • Birthweight is most reliable indicator of infant’s health • Weight prior to conception • Influences fetal growth • Underweight • Higher rates of preterm births and infant deaths • Overweight & obesity • Higher risk of their own medical complications- hypertension, gestational DM, postpartum infections, • Risks for infant- NTD from maternal poor glycemic control, heart defects and other abnormalities, infant wt >9 lbs from diabetic mother- caesarean section
Maternal Weight • Weight gain during pregnancy- only 1/3 gain the right amount; most gain more • Fetal growth and maternal health • Correlates closely with infant birthweight • Predictor of health and development • Recommended weight gains- see the chart • Number of fetuses • Beginning weight
Maternal Weight • Weight gain patterns • 3.5 pounds in first trimester • 1 pound per week thereafter • Large weight gain over short time • Preeclampsia • Components of weight gain • Placenta, uterus, blood, breasts, fluid volume, baby • Maternal fat stores
Increase in breast size 2 Increase mother's fluid volume 4 Placenta 1 1/2 Increase in blood supply to the placenta 4 Amniotic fluid 2 Infant at birth 7 1/2 Increase in size of uterus and supporting muscles 2 Mother's necessary fat stores 7 1st trimester 2nd trimester 3rd trimester 30 Weight gain (lb) Stepped Art
Maternal Weight • Weight loss after pregnancy • Return to prepregnancy weight • Ideal but not typical • Retain a couple of pounds fat with each pregnancy • Seven or more pounds, BMI increased 1 unit risks diabetes and hypertension • Chronic diseases later in life for mother and infant • Losing the pregnancy weight indicates better success at maintaining middle age weight
Exercise During Pregnancy • Can continue “moderate intensity” exercise throughout pregnancy 30 min/session • Do regularly and adjust duration and intensity as needed • “Low-impact” activities like swimming, walking • Benefits • Less diabetes, easier labor • Protect fetal development with Exercise “Don’ts” • Stay out of saunas, hot humid weather. • Keep hydrated Don’t push yourself. • No contact sports No exercise on your back • Stop if painful No bouncy jerky exercise
DO DON’T Do begin to exercise gradually. Don’t exercise vigorously after long periods of inactivity. Do exercise regularly (most, if not all, days of the week). Don’t exercise in hot, humid weather. Do warm up with 5 to 10 minutes of light activity. Don’t exercise when sick with fever. Do 30 minutes or more of moderate physical activity; 20 to 60 minutes of more intense activity on 3 to 5 days a week will provide greater benefits. Don’t exercise while lying on your back after the first trimester of pregnancy or stand motionless for prolonged periods. Pregnant women can enjoy the benefits of exercise. Do cool down with 5 to 10 minutes of slow activity and gentle stretching. Don’t exercise if you experience any pain, discomfort, or fatigue. Do drink water before, after, and during exercise. Don’t participate in activities that may harm the abdomen or involve jerky, bouncy movements. Safe exercise during pregnancy Do eat enough to support the needs of pregnancy plus exercise. Do rest adequately.
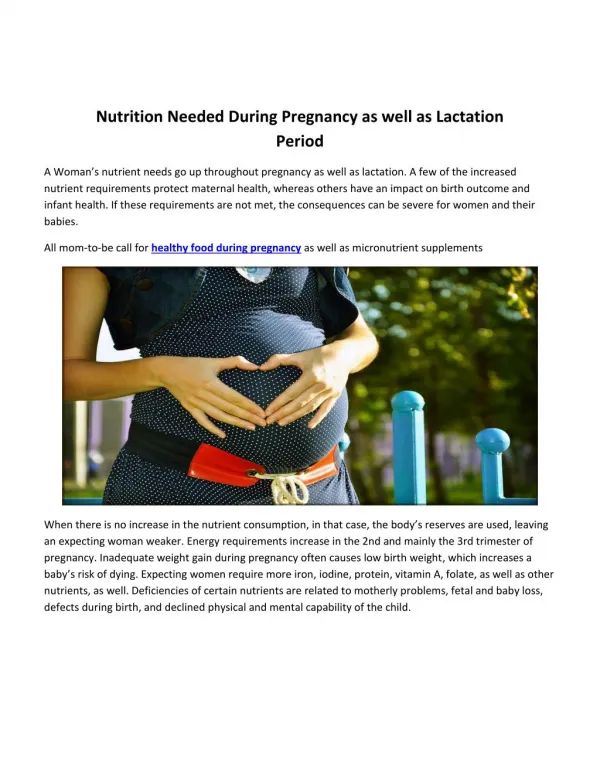
Energy & Nutrient Needs During Pregnancy • Nutrient needs tend to be higher than any other time in life. • To meet needs • Make nutrient-dense selections • Body maximizes absorption, minimizes losses • Fe, folate, Ca especially important
Energy & Nutrient Needs During Pregnancy • Energy • Increase in basal metabolic rate • 1st trimester- usual kcal, focus on getting ALL micronutrients • 2nd trimester add 340 kcal/d • 3rd trimester add 450 kcal/d • Food energy • Need 15 to 20% more energy than before pregnancy • Nutrient-dense foods
Energy & Nutrient Needs During Pregnancy • Carbohydrate • Ample carbohydrate is necessary • Protein • RDA – additional 25 grams per day • Essential fatty acids • Omega-3 and omega-6 fatty acids needed for developing brain material (make a smart baby now)
Energy & Nutrient Needs During Pregnancy • Fetal blood production and cell growth (DNA) and maternal red blood cell mass • Folate 600 μg/d • Vitamin B12 2.6 μg/d • Iron 27 mg/d • Zinc 12 mg/d • Benefits of prenatal supplements: Drugstore prenatal OK • Intentionally eat well. The pill can only do so much.
Energy & Nutrient Needs During Pregnancy • Nutrients for bone development • Protect your own bones from “borrowing” • Vitamin D • Deficiency interferes with calcium metabolism • Calcium • Absorption and retention increase • Intake usually falls below recommendations • Other nutrients • Optimal interval between pregnancies
Vegetarian Diets During Pregnancy & Lactation • Can support healthy pregnancy and lactation • Must be planned and disciplined • Should include dairy and eggs • Variety of whole foods • Additional supplementation- B12, Fe, Ca, D • Focus on COMPLETE proteins (complementary) • Vegan diets – NO!! NO!! NO!! NO!!! • Risks- too many to list, long-term and irreversible effects a real potential
Common Nutrition-Related Concerns of Pregnancy • Nausea • “Morning sickness” to can’t keep anything down • Try a 50 mg B6 pill from weeks 6-14 • http://www.morningsicknesshelp.com/morning-sickness-cure.html • Constipation and hemorrhoids • Heartburn • Food cravings and aversions • Hormone-induced changes • Nonfood cravings- pica
High-Risk Pregnancies • Infant’s birthweight • Low birthweight (LBW) • 5 ½ pounds or less • Risk of complications • Relationship with socioeconomic status • Gestational age • Preterm • Small-for-gestational age
High-Risk Pregnancies • Malnutrition and pregnancy • Fertility • Early, unplanned pregnancy • Poor placental development can affect fetus’s future children • Fetal development • Consequences • Retardation, birth defects, miscarriages, stillbirths, infant mortality 0-4 yrs.
High-Risk Pregnancies • Food Assistance Programs • WIC • Nutrition education and nutritious foods • Vulnerable populations who qualify for help • Cost-benefit • Remedial and preventive services
High-Risk Pregnancies • Maternal age • Ideal childbearing age 20-25, up to 35 yrs OK • Adolescents • Risk of pregnancy complications • Higher rates of stillbirths, preterm births, and LBW infants • Weight gain recommendations • Imperative need to seek prenatal care
High-Risk Pregnancies • Maternal age • Women older than 35 yrs • Complications often reflect chronic conditions • Cesarean section rates increase • Maternal death rates are higher • Risks for fetus • Down’s syndrome 1/100 for 40 yr old vs. 1/10,000 for 20 yr old
High-Risk Behaviors • Alcohol consumption • Irreversible mental and physical retardation • Fetal alcohol syndrome (FAS) • Medicinal drugs • No medication use without consulting physician • Herbal supplements • Seek physician advice