Download
1 / 66
1.31k likes | 5.06k Views
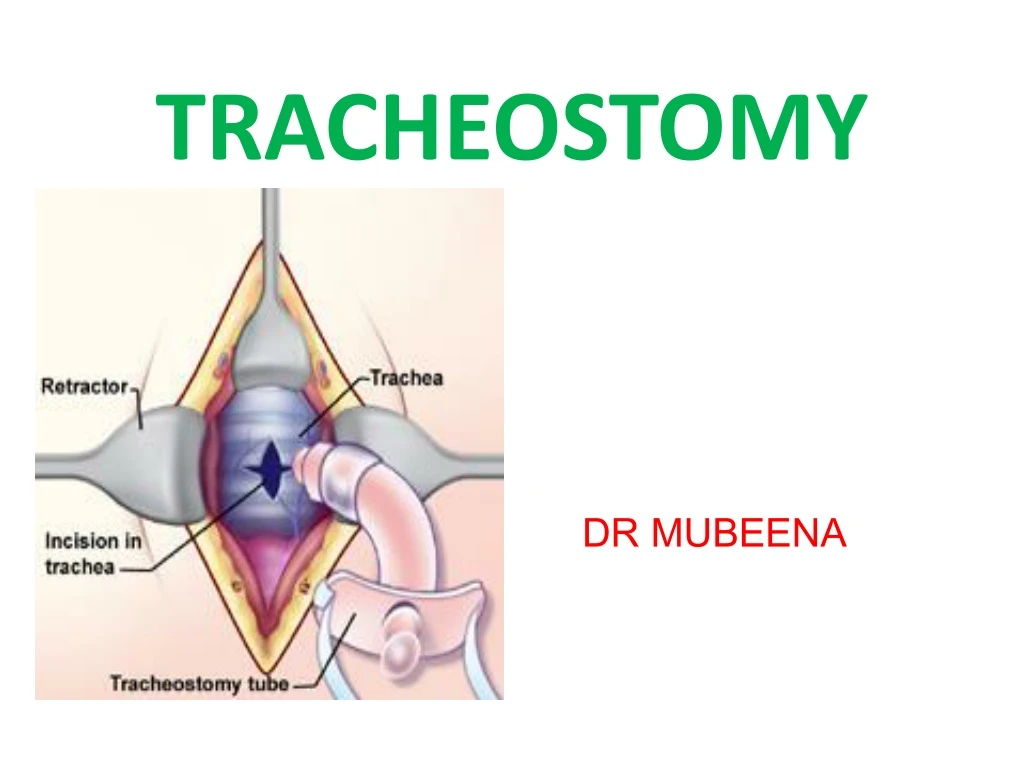
TRACHEOSTOMY. DR MUBEENA. Definition. A tracheostomy is a surgically created airway by making a hole in the anterior wall of the trachea and converting it into a stoma on the skin surface Derived from Greek words ‘ tracheia arteria ’- rough artery. Functions of Tracheostomy.

E N D
TRACHEOSTOMY DR MUBEENA
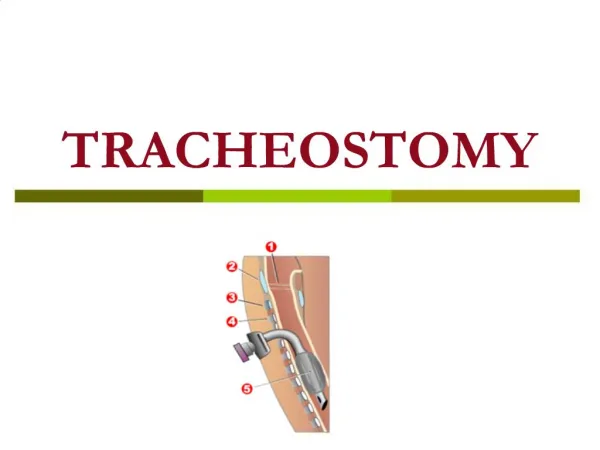
Definition • A tracheostomy is a surgically created airway by making a hole in the anterior wall of the trachea and converting it into a stoma on the skin surface • Derived from Greek words ‘tracheiaarteria’- rough artery
Functions of Tracheostomy 1. Alternative pathway for breathing 2. Improves alveolar ventilation In cases of respiratory insufficiency: (a) Decreasing the dead space by 30-50% (normal dead space is 150 ml). (b) Reducing the resistance to airflow. 3. Protects the airways 4. Permits removal of tracheobronchial secretions 5. Intermittent positive pressure respiration (IPPR) If IPPR is required beyond 72 hours, tracheostomy is superior to intubation. 6. To administer anaesthesia laryngopharyngeal growths or trismus.
Indications of Tracheostomy There are three main indications A. Respiratory obstruction. B. Retained secretions. C. Respiratory insufficiency.
A. Respiratory obstruction 1. Infections Acute laryngo-tracheo-bronchitis, acute epiglottitis, diphtheria, Ludwig's angina, peritonsillar, retropharyngeal or parapharyngeal abscess, tongue abscess 2. Trauma External injury of larynx and trachea ,Trauma due to endoscopies, especially in infants and children,Fracturesof mandible or maxillofacial injuries 3. Neoplasms Benign and malignant neoplasms of larynx, pharynx, upper trachea, tongue and thyroid 4. Foreign body larynx 5. Oedema larynx due to steam, irritant fumes or gases, allergy (angioneurotic or drug sensitivity), radiation 6. Bilateral abductor paralysis 7. Congenital anomalies • Laryngeal web, cysts, tracheo-oesophageal fistula Bilateral choanal atresia
B. Retained secretions 1. Inability to cough • Coma of any cause, e.g. head injuries, cerebrovascular accidents, narcotic overdose • Paralysis of respiratory muscles, e.g. spinal injuries, polio, Guillain-Barre syndrome, myasthenia gravis • Spasm of respiratory muscles, tetanus, eclampsia, strychnine poisoning 2. Painful cough • Chest injuries, multiple rib fractures, pneumonia 3. Aspiration of pharyngeal secretions • Bulbar polio, polyneuritis, bilateral laryngeal paralysis
C. Respiratory insufficiency • Chronic lung conditions, viz. emphysema, chronic bronchitis, bronchiectasis, atelectasis.
Types of Tracheostomy • Emergency tracheostomy • Elective or tranquil tracheostomy • Permanent tracheostomy • Percutaneous dilatational tracheostomy • Mini tracheostomy (cricothyroidotomy)
1. Emergency tracheostomy • It is employed when airway obstruction is complete or almost complete and • There is an urgent need to establish the airway. • Intubation or laryngotomyare either not possible or feasible in such cases.
2. Elective tracheostomy(syn. tranquil, orderly or routine tracheostomy) • This is a planned, unhurried procedure. Almost all operative surgical facilities are available, endotracheal tube can be put and local or general anaesthesia can be given. • It is of two types: (a) Therapeutic: to relieve respiratory obstruction, remove tracheobronchial secretions or give assisted ventilation. (b) Prophylactic: to guard against anticipated respiratory obstruction or aspiration of blood or pharyngeal secretions such as in extensive surgery of tongue, floor of mouth, mandibular resection or laryngofissure.
3. Permanent tracheostomy • Required for case of bilateral abductor paralysis or laryngeal stenosis.
BASED ON LEVEL (THYROID isthmus lies against II, III and IV tracheal rings). above the level of thyroid isthmus perichondritis of the cricoid cartilage It is always avoided. Only indication - carcinoma of larynx preferred one Throughthe II or III rings below the level of isthmus. Trachea is deep at this level and close to several large vessels; also there are difficulties with tracheostomy tube which impinges on suprasternal notch.
Technique • Whenever possible, endotracheal intubation should be done before tracheostomy. This is specially important in infants and children. • Position Supine with a pillow under the shoulders so that neck is extended.
Anaesthesia 2 % lignocaine & 1 in 2 lakh adrenaline injected into incision line
A transverse incision, 5 cm long, made 2 fingers' breadth above the sternal notch can be used in elective procedures. It has the advantage of a cosmetically better scar .
1. A vertical incision in the midline of neck, extending from cricoid cartilage to just above the sternal notch.
2. After incision, tissues are dissected in the midline. Dilated veins are either displaced or ligated.
3. Strap muscles are separated in the midline and retracted laterally.
4. Thyroid isthmus is displaced upwards or divided between the clamps, and suture-ligated.
Confirmation of trachea • 5 ml syringe containing 4 % Lignocaine taken, its needle inserted into trachea & aspirated. Air bubbles confirm presence of needle in trachea. • 2 ml of solution injected into trachea & needle removed quickly to avoid breaking of needle during violent cough movements.
. Trachea is fixed with a hook and opened with a vertical incision in the region of 3rd and 4th or 3rd and 2nd rings. This is then converted into a circular opening. The first tracheal ring is never divided as perichondritis of cricoid cartilage with stenosis can result
6. Tracheostomy tube of appropriate size is inserted and secured by tapes Lubricated tracheostomy tube inserted into trachea Confirm presence of tube in trachea with help of ambu bag & auscultation
7. Skin incision should not be sutured or packed tightly as it may lead to development of subcutaneous emphysema. 8. Gauze dressing is placed between the skin and flange of the tube around the stoma
9.Tapes of tracheostomy tube tied around the neck keeping a space for 1 finger. Neck kept flexed. Skin incision closed loosely to avoid surgical emphysema.
Insertion of medicated gauze Betadine soaked gauze or Sofratulle put around the tracheostomy opening.
Portex cuffed tube • Made of siliconized Poly Vinyl Chloride. It is thermolabile & prevents crusting. • Low pressure high volume cuff maintains an air-tight seal required for: • Prevention of aspiration of secretions • Positive pressure ventilation
Jackson’s metallic tube • Made of German silver (alloy of Ag + Cu + P) • Has obturator (pilot), inner tube & outer tube • Inner tube is longer than outer tube for its removal & cleaning. Outer tube maintains patency. Pilot is inserted into outer tube for smooth & non-traumatic insertion of tube • Lock prevents expulsion of tube during cough
Fuller’s metallic tube • Outer tube bi-valved. The 2 blades when pressed together, help in smooth entry of tube. • Inner tube is longer & has a vent for phonation • Pt phonates by closing main tube opening • Vent also helps in decannulation of tube
TYPES OF TRACHEOSTOMYTUBES • Plastic or metal • Cuffed or uncuffed • Fenestrated or unfenestrated • Double canula or single canula
PaediatricTracheostomy -Soft and compressible trachea ,so difficult to identify and may get displaced & injure recurrent laryngeal nerve -Preferably in general anaesthesia -Don’t extend neck too much as pleura,innominatevessels,thymus may get injured -Post operative x-ray of the neck to know position of the tube -Use of soft silastic and portex tube
Post Operative Care 1.Constant Supervision • For bleeding, displacement, blocking of tubes, removing secretions • Patient is given a bell or paper pad to communicate • Pt given 100 % oxygen. Deflate the tube cuff.
3.Tracheostomy tube care • Inner tube is removed & cleaned when blocked • Outer tube never removed before 72 hrs to allow formation of tracheo-cutaneous tract • Cuff of Portex tube deflated for 10 minutes every 2 hours to prevent pressure necrosis & dilatation of trachea
4. Others • Chest auscultated for confirmation of adequate suctioning. Re-inflate cuff to a pressure of 25 mmHg. Patient oxygenated again. • Tracheostomy wound dressing done BID • Steam inhalation TID. Moist gauze piece placed over tracheostomy tube opening. Regular chest physiotherapy, expectorants & mucolytics given.
5.Prevention of crusting and tracheitis -Proper humidification using humidifier,nebulizer -Using a few drops of ringer lactate or normal saline or hypotonic saline -Every 2-3 hrs
Decannulation • Adult: plug or seal tube opening & if tolerated for 24 hrs, remove tube. • Child: Sequentially reduce size of tube. After tube removal close wound. Healing occurs within 1 week. Secondary closure after freshening the wound margin is required rarely. • Infant or a young child -Decannulate in operation theatre -Equipment for re-intubation should ne available like good headlight, laryngoscope, proper sized endotracheal tubes and a tracheostomy tray -After decannulation observe for respiratory distress,tachycardia, colour. -Oximetry is useful
Decannulation difficulty Organic causes Non-organic causes: Emotional dependence in children Inability to tolerate upper airway resistance • Persistence of cause requiring tracheostomy • Obstructing tracheal granulations • Tracheal oedema • Subglottic stenosis • Collapse of tracheal wall (tracheomalacia)
Complications of tracheostomy • Immediate Complications (During tracheostomy) • Intermediate Complications (Few hours or days later) • Late Complications (Due to prolonged use of tube for weeks-months)
Immediate complications • Haemorrhage • Aspiration of blood • Injury to recurrent laryngeal nerve • Injury to apical pleura (Pneumothorax) • Injury to oesophagus (May cause tracheoesophageal fistula) • Apnoea (Due to Carbondioxide wash out)
Intermediate Complications • Haemorrhage • Displacement of tube (Due to use of improper size tube) • Blocking of tube (Due to excessive crusting/poor humidification) • Subcutaneous emphysema • Tracheitis/Tracheobronchitis with crusting in trachea • Pulmonary infections (Due to compromised airway defense mechanism) • Wound infection & granulation
Late Complications • Haemorrhage (Due to erosion of major vessels espinnominate/bracheocephalic art) • Laryngeal stenosis (Due to perichondritis of cricoid cartilage) • Tracheal stenosis (Due to tracheal ulceration & infection) • Tracheoesophageal fistula (Due to erosion of trachea by tip of the tube) • Persistent tracheocutaneous fistula • Keloid/Unsighty scar at tracheostomy site • Difficult decannulation
Procedure for immediate airway management • Jaw thrust • Lifting the jaw forward & extensing the neck • Improves airway by displacing the soft tissues • Avoided in spinal injuries