Download
1 / 41
420 likes | 450 Views
Juvenile Idiopathic Arthritis. Prof ImranIqbal Prof of Paediatrics (2003-2018). In the name of ALLAH the most Gracious, the most Merciful. Juvenile Idiopathic Arthritis (JIA). Age < 16 yrs Duration > 6 wks Joint Inflammation -- pain or tenderness -- heat

E N D
Juvenile Idiopathic Arthritis Prof ImranIqbal Prof of Paediatrics (2003-2018)
In the name of ALLAH the most Gracious, the most Merciful
Juvenile Idiopathic Arthritis (JIA) • Age < 16 yrs • Duration > 6 wks • Joint Inflammation -- pain or tenderness -- heat -- swelling or effusion -- limited range of motion
EPIDEMIOLOGY • Prevalence : estimated between 57 and 113 per 100,000 children. • Annual incidence: 2 to 20 per 100,000 children.
ETIOLOGY • Genetic factors - cytokine levels • Environmental factors – infections • Immune system dysregulation
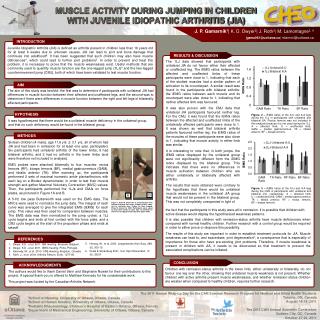
Fever Joint Inflammation Anemia Lancet 1995 Blood 1996 J Exp Med 1998 A&R 1991 Growth Impairment Interleukin-6 in sJIA Thrombocytosis A&R 1991 J Clin Invest 1997 Endocrinol 2001 IL-6/soluble IL-6R and CRP Osteoporosis MAS A&R 2006 J Clin Invest 1994
AGE • Birth – 16 yrs • Mean age – 7 yrs Jamal Raza et al, A cross sectional study on juvenile idiopathic arthritis in paediatric population; J Pak Med Assoc; Vol. 65, No. 4, April 2015
JIA - Classification • Oligoarthiritis • Polyarthritis • Systemic arthiritis • Psoriatic arthiritis • Enthesitis – related arthiritis • Undifferentiated arthiritis
JIA - Classification • Oligoarthiritis -- Joints 4 or < 4 -- usually ankles or knees • -- Persistent • -- Extended - > 4 after 6 months
JIA - Classification • Polyarthiritis -- Joints > 4 -- large and small joints -- usually all limbs • -- Rheumatoid factor + ve • -- Rheumatoid factor – ve
JIA - Classification • Systemic onset -- Joints – 1 or more -- Fever - 14 days or more -- one of the following signs • -- Erythematous rash • -- Hepatosplenomegaly • -- Generalized Lymphadenapathy • -- Serositis
JIA - Types • Polyarticular 71.9% • Oligoarticular 22.7% • Systemic JIA 5.4% • RF positive 10.27% JCPSP 2013 Vol 23(6): 409-412
The frequency and classification of juvenile idiopathic arthritis (JIA) subtypes JIA Systemic4–17% Oligoarticular 27–56% Polyarticular 18–30% Psoriatic2–11% Enthesitis 3–11% Undifferentiated 10% Persistent 25–35% Extended 15–20% RF (+) 2–7% RF (–) 11–28% Petty RE, et al.J Rheumatol 2004; 31:390–392. Ravelli A & Martini A. Lancet 2007; 369:767–778. Goldzweig O & Hashkes PJ. Drug Des Devel Ther 2011; 5:61–70. RF (+) = rheumatoid factor positive RF (–) = rheumatoid factor negative
Spondyloarthritis Enthesitis-related JIA Enthesis: insertion of ligaments and tendons into bone Asymmetrical arthritis affects 4 or fewer joints Male predominance, Age>8 years. +ve Family H/O HLA B-27 related disease Anterior or Acute Iritis
Ankylosing spondylitis • Enthesitis of axial skeleton and sacroiliac joints. • Present with back pain • Loss of lumbosacral mobility • Oligoarthritis of joints of lower extremities • Male to Female ratio 7:1 • Common presentation • Male with back pain, morning stiffness that is relieved w/ exercise
Diagnosis • Joint pain, swelling • Limitation of movement • Morning stiffness • Limp in walk • Fever • Anorexia, FTT
Common Differential Diagnosis • Rheumatic fever • Reactive arthiritis • Causes of PUO • Sickle cell disease • Acute Leukemia • Farber disease
Lab investigations • CBC • ESR , CRP • RF / ANA • Serum Ferritin • X- rays • MRI
JIA – Goals of Treatment • Early Control of disease • Relieve discomfort • Prevent joint damage • Avoid drug toxicity • Maintain physical function • Improve the quality of life
JIA – Multidisciplinary Treatment • Medications • Consultations • Physiotherapy • Occupational therapy • Nutrition • Education • Psychosocial support
JIA – Therapeutics • NSAIDs -- Naproxen • DMARDs -- Methotrexate • Biologic agents -- Tocilizumab
NSAIDs • Inhibit prostaglandin synthesis • Relieve pain • Decrease inflammation • Take 4 weeks for full effect • Do not affect course of disease • GI and renal toxicity
DMARDs • Inhibit cytokine production • Decrease lymphocyte proliferation • Effect builds in 6-12 weeks • Steroid sparing agents • Modify long term course of disease • Blood and liver toxicity
Corticosteroids • Powerful agents to reduce inflammation • Affect the immune system • Decrease lymphocyte proliferation • Helpful in initial control of disease • Prolonged use produces toxicity • Adverse Effects - Cusingoid features, hypertension, mood disturbances, glucose intolerance, osteoporosis, growth suppression, infections
Biologic Agents • Recently developed • Target specific cytokines • TNF / Interleukin antagonists • Given IV or SC • Effective in resistant cases • Increased infections
Fever Joint Inflammation Anemia Lancet 1995 Blood 1996 J Exp Med 1998 A&R 1991 Growth Impairment Interleukin-6 in sJIA Thrombocytosis A&R 1991 J Clin Invest 1997 Endocrinol 2001 IL-6/soluble IL-6R and CRP Osteoporosis MAS A&R 2006 J Clin Invest 1994
Tocilizumab • IL -6 antagonist • Useful in systemic and polyarthiritis JIA • Given IV every 2-4 wks • Improvement seen in 12 wks
Children Hospital & Institute of Child Health, Multan, Pakistan