Download
1 / 1
50 likes | 674 Views
A NOVEL EARLY PREGNANCY ASSESSMENT UNIT/GYNAECOLOGY ASSESSMENT UNIT DASHBOARD AN EXPERIENCE FROM A UK DISTRICT GENERAL HOSPITAL K.WAHBA, A.SHAH, K.HILL EARLY PREGNANCY ASSESSMENT UNIT,YEOVIL DISTRICT HOSPITAL,UK. Introduction

E N D
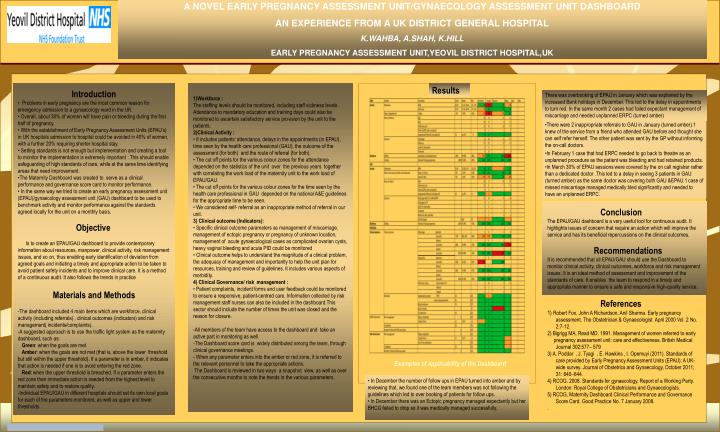
A NOVEL EARLY PREGNANCY ASSESSMENT UNIT/GYNAECOLOGY ASSESSMENT UNIT DASHBOARD AN EXPERIENCE FROM A UK DISTRICT GENERAL HOSPITAL K.WAHBA, A.SHAH, K.HILL EARLY PREGNANCY ASSESSMENT UNIT,YEOVIL DISTRICT HOSPITAL,UK Introduction • Problems in early pregnancy are the most common reason for emergency admission to a gynaecology ward in the UK. • Overall, about 30% of women will have pain or bleeding during the first half of pregnancy. • With the establishment of Early Pregnancy Assessment Units (EPAU’s) in UK hospitals admission to hospital could be avoided in 40% of women, with a further 20% requiring shorter hospital stay. • Setting standards is not enough but implementation and creating a tool to monitor the implementation is extremely important .This should enable safeguarding of high standards of care, while at the same time identifying areas that need improvement. • The Maternity Dashboard was created to serve as a clinical performance and governance score card to monitor performance. • In the same way we tried to create an early pregnancy assessment unit (EPAU)/gynaecology assessment unit (GAU) dashboard to be used to benchmark activity and monitor performance against the standards agreed locally for the unit on a monthly basis. Objective Is to create an EPAU/GAU dashboard to provide contemporary information about resources, manpower, clinical activity, risk management issues, and so on, thus enabling early identification of deviation from agreed goals and initiating a timely and appropriate action to be taken to avoid patient safety incidents and to improve clinical care. It is a method of a continuous audit. It also follows the trends in practice Materials and Methods -The dashboard included 4 main items which are workforce, clinical activity (including referrals) , clinical outcomes (indicators) and risk management( incidents/complaints). -A suggested approach is to use the traffic light system as the maternity dashboard, such as: Green: when the goals are met Amber: when the goals are not met (that is, above the lower threshold but still within the upper threshold). If a parameter is in amber, it indicates that action is needed if one is to avoid entering the red zone. Red: when the upper threshold is breached. If a parameter enters the red zone then immediate action is needed from the highest level to maintain safety and to restore quality. -Individual EPAU/GAU in different hospitals should set its own local goals for each of the parameters monitored, as well as upper and lower thresholds 1)Workforce : The staffing levels should be monitored, including staff sickness levels . Attendance to mandatory education and training days could also be monitored to ascertain satisfactory service provision by the unit to the patients. 2)Clinical Activity : • It includes patients’ attendance, delays in the appointments (in EPAU), time seen by the health care professional (GAU), the outcome of the assessment (for both) and the route of referral (for both). • The cut off points for the various colour zones for the attendance depended on the statistics of the unit over the previous years together with correlating the work load of the maternity unit to the work load of EPAU/GAU. • The cut off points for the various colour zones for the time seen by the health care professional in GAU depended on the national A&E guidelines for the appropriate time to be seen. • We considered self- referral as an inappropriate method of referral in our unit. 3) Clinical outcome (Indicators): • Specific clinical outcome parameters as management of miscarriage, management of ectopic pregnancy or pregnancy of unknown location, management of acute gynaecological cases as complicated ovarian cysts, heavy vaginal bleeding and acute PID could be monitored • Clinical outcome helps to understand the magnitude of a clinical problem, the adequacy of management and importantly to help the unit plan for resources, training and review of guidelines. It includes various aspects of morbidity. 4) Clinical Governance/ risk management : • Patient complaints, incident forms and user feedback could be monitored to ensure a responsive, patient-centred care. Information collected by risk management staff nurses can also be included in the dashboard.This sector should include the number of times the unit was closed and the reason for closure. -All members of the team have access to the dashboard and take an active part in monitoring as well. -The Dashboard score card is widely distributed among the team, through clinical governance meetings. - When any parameter enters into the amber or red zone, it is referred to the relevant personnel to take the appropriate actions. The Dashboard is reviewed in two ways a snapshot view, as well as over the consecutive months to note the trends in the various parameters. Results There was overbooking of EPAU in January which was explained by the increased Bank holidays in December. This led to the delay in appointments to turn red. In the same month 2 cases had failed expectant management of miscarriage and needed unplanned ERPC (turned amber) There were 2 inappropriate referrals to GAU in January (turned amber).1 knew of the service from a friend who attended GAU before and thought she can self refer herself. The other patient was sent by the GP without informing the on-call doctors. In February 1 case that had ERPC needed to go back to theatre as an unplanned procedure as the patient was bleeding and had retained products. In March 30% of EPAU sessions were covered by the on call registrar rather than a dedicated doctor .This led to a delay in seeing 3 patients in GAU (turned amber) as the same doctor was covering both GAU &EPAU.1 case of missed miscarriage managed medically bled significantly and needed to have an unplanned ERPC. Conclusion The EPAU/GAU dashboard is a very useful tool for continuous audit. It highlights issues of concern that require an action which will improve the service and has its beneficial repercussions on the clinical outcomes. Recommendations It is recommended that all EPAU/GAU should use the Dashboard to monitor clinical activity, clinical outcomes, workforce and risk management issues. It is an ideal method of assessment and improvement of the standards of care. It enables the team to respond in a timely and appropriate manner to ensure a safe and responsive high-quality service. References 1) Robert Fox, John A Richardson, Anil Sharma. Early pregnancy assessment. The Obstetrician & Gynaecologist April 2000 Vol. 2 No. 2:7-12. 2) Bigrigg MA, Read MD. 1991. Management of women referred to early pregnancy assessment unit: care and effectiveness. British Medical Journal 302:577– 579 3) A. Poddar , J. Tyagi , E. Hawkins , I. Opemuyi (2011). Standards of care provided by Early Pregnancy Assessment Units (EPAU): A UK-wide survey. Journal of Obstetrics and Gynaecology, October 2011; 31: 640–644. 4) RCOG. 2008. Standards for gynaecology. Report of a Working Party. London: Royal College of Obstetricians and Gynaecologists. 5) RCOG, Maternity Dashboard Clinical Performance and Governance Score Card. Good Practice No. 7 January 2008. . Examples of applicability of the Dashboard • In December the number of follow ups in EPAU turned into amber and by reviewing that, we found one of the team members was not following the guidelines which led to over booking of patients for follow ups. • In December there was an Ectopic pregnancy managed expectantly but her BHCG failed to drop so it was medically managed successfully.