Download

1 / 66
1.75k likes | 4.71k Views
Partograph. Prof. Ashis Kumar Mukhopadhyay Professor, G & O Medical Superintendent-cum-Vice Principal CSS College of Obstetrics & Gynaecology, Kolkata National Chairperson, Medical Education Committee of FOGSI. Partograph:

E N D
Prof. Ashis Kumar Mukhopadhyay Professor, G & O Medical Superintendent-cum-Vice Principal CSS College of Obstetrics & Gynaecology, Kolkata National Chairperson, Medical Education Committee of FOGSI
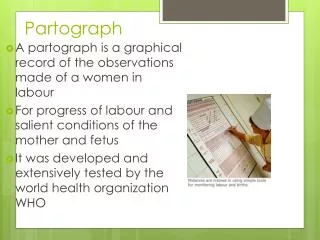
Partograph: First introduced by Freidman in New York in 1954. It is the graphic analysis of labor for clinical evaluation of the program in labor and the simplest form of it plots the dilatation of cervix in centimeter against time in labour.
Modification by Phillpot and Castle (1972 ): Phillpot and castle added alert line and Action line to the graph with material advantage for clinical management. They also measured descent of the presenting part, while measuring dilatation of the cervix P/V and in relation to ischial spines (the station) excluding caput formation and moulding of foetal head. The simple and neglected assessment of measuring the head in fifths by abdominal examination is the more valid and reliable method of progress.
WHO multicentric study (1994) 35484 women (South-East Asia) % % Labor > 18 hrs 6.4 to 3.4 Augmentation 20.7 to 9.1 Emergency C.Section 19 to 16 Augmentation by 54% C. Section for CPD by 62%
WHO multicentric study (1994) • in mean no. of • vaginal examination • postpartum sepsis • Effects seen in nulliparous and parous women • total stillbirth 2.8% to 2.4% • IP stillbirth 0.50% to .31% • early neonatal death 0.5% to 0.3%
Partogram • Reduction in maternal morbidity • Reduction in perinatal mortality and morbidity
W.H.O • Recommended Partograph in all labour cases which has reduced the incidence of prolonged labour and LUCS with improvement of maternal morbidity,foetal morbidity and mortality. • Took out a model composite partograph in 1988 for developing countries.
Using the Partograph • Patient information: Name, gravida, para, hospital regn number, date and time of admission, and time of ruptured membranes • Fetal heart rate: Record every half hour • Amniotic fluid: Record the color at every vaginal examination • I : membranes intact • C: membranes ruptured, clear fluid • M: meconium-stained fluid • B: blood-stained fluid
Using the Partograph …cont. • Moulding: • sutures apposed • sutures overlapped but reducible • sutures overlapped and not reducible • Cervical dilatation: Assess at every vaginal examination, mark with cross (X) • Alert line: Line starts at 4 cm of cervical dilatation to the point of expected full dilatation at the rate of 1 cm per hr • Action line: Parallel and 4 hours to the rt of the alert line
Using the Partograph …cont. • Hours: Time elapsed since onset of active phase of labor (observed or extrapolated) • Time: Record actual time • Contractions: Chart every half hour; palpate the number of contractions in 10 minutes and their duration in seconds • Less than 20 seconds: • Between 20 and 40 seconds: • More than 40 seconds: • Oxytocin: Record amount per volume IV fluids in drops/min. every 30 min. when used • Drugs given: Record any additional drugs given
The Partograph • Assessment of fetal well being • Assessment of maternal well being • Assessment of progress of labor
Measuring Fetal Well Being During Labor • Fetal heart rates and pattern • Degree of moulding, caput • Color of amniotic fluid
Components of the partograph • Part I : fetal condition ( at top ) • Part II : progress of labour ( at middle ) • Part III : maternal condition ( at bottom ) • Outcome ………………
Part 1 : Fetal condition • This part of the graph is used to monitor and assess fetal condition • 1 - Fetal heart rate • 2 - membranes and liquor • 3 - moulding the fetal skull bones • Caput
Fetal heart rate Basal fetal heart rate? • < 160 beats/mi =tachycardia • >120 beats/min = bradycardia • >100beats/min = severe bradycardia Decelerations? yes/no Relation to contractions? • Early • Variable • Late – -----Auscultation - return to baseline > 30 sec contraction ----- Electronic monitoring peak and trough (nadir) > 30 sec
Membranes and liquor • intact membranes ………….I • ruptured membranes + clear liquor …….C • ruptured membranes + meconium- stained liquor ….M • ruptured membranes + blood – stained liquor …B • ruptured membranes + absent liquor…………………....A
Moulding the fetal skull bones • Molding is an important indication of how adequately the pelvis can accommodate the fetal head • increasing molding with the head high in the pelvis is an ominous sign of cephalopelvic disproportion • separated bones . sutures felt easily ……………….….O • bones just touching each other ………………………..+ • overlapping bones ( reducible 0 ……………………...++ • severely overlapping bones ( non – reducible ) ……..+++
Measuring Maternal Well Being During Labor • Pulse, temperature, blood pressure, respiration • Urine output, ketones, protein
Part II – progress of labour Cervical diltation • Descent of the fetal head • Fetal position • Uterine contractions • This section of the paragraph has as its central feature a graph of cervical diltation against time • it is divided into a latent phase and an active phase
Latent phase : • it starts from onset of labour until the cervix reaches 3 cm diltation • once 3 cm diltation is reached , labour enters the active phase • lasts 8 hours or less • each lasting < 20 sceonds • at least 2/10 min contractions
Active phase : • Contractions at least 3 / 10 min • each lasting < 40 seconds • The cervix should dilate at a rate of 1 cm / hour or faster
Alert line ( health facility line ) • The alert line drawn from 3 cm diltation represents the rate of diltation of 1 cm / hour • Moving to the right or the alert line means referral to hospital for extra vigilance
Action line ( hospital line ) • The action line is drawn 4 hour to the right of the alert line and parallel to it • This is the critical line at which specific management decisions must be made at the hospital
Descent of the fetal head • Descent assessed by abdominal palpation: Part of head (divided into 5 parts) palpable above the symphysis pubis; recorded as a circle (O) at every vaginal examination. At 5/5 whole of the fetal head is palpable above symphysis pubis; At 0/5, entire head has gone inside true pelvis.
Using the Partograph (contd.) • Temperature: Record every 2 hours • Pulse: Record every 30 minutes and mark with a dot (•) • Blood pressure: Record every 4 hours and mark with arrows • Protein, acetone and volume: Record every time urine is passed
Cervical diltation • It is the most important information and the surest way to assess progress of labour , even though other findings discovered on vaginal examination are also important • when progress of labour is normal and satisfactory , plotting of cervical diltation remains on the alert line or to left of it • if a woman arrives in the active phase of labour , recording of cervical diltation starts on the alert line • when the active phase of labor begins , all recordings are transferred and start by pltting cervical diltation on the alert line
Primary Dysfunctional Labour cervical dilatation < 1 cm / hr in active phase Secondary Arrest Normal progress in early active phase but slow or no cervical dilatation later
Partograph Showing Inadequate Uterine Contractions Corrected with Oxytocin
Advantages: • Single sheet of paper with all information. • No need to record labor events repeatedly. • Predict deviation from normal duration of labour – proper intervention could be done in time. • Facilitates hand over and responsibility and accountability of the person conducting labour. • Simplifies transfer of labour patients to FRU. • A very good medicolegal document.
That’s all for now! Thank you
STEP 1 Mrs. A. was admitted at 05.00 on 12.5.2008 Membranes ruptured 04.00 Gravida 3, Para 2+0 Hospital number 7886 On admission the fetal head was 4/5 palpable above the symphysis pubis and the cervix was 2 cm dilated Q: What should be recorded on the partograph?
A: The woman is not in active labour. Record only the details of her history, not the descent and cervical dilatation.
STEP 2 09.00: The fetal head is 3/5 palpable above the symphysis pubis The cervix is 5 cm dilated
A: The woman is now in the active phase of labor. Plot this and the following information on the partograph: There are 3 contractions in 10 minutes, each lasting 20–40 seconds Fetal heart rate (FH) 120 Membranes ruptured, amniotic fluid clear Sutures of the skull bones are apposed
Blood pressure 120/70 mm Hg • Temperature 36.8°C • Pulse 80 per minute • Urine output 200 mL; negative • protein and acetone
Q: What should you now record on the partograph? Q: What steps should be taken? Q: What advice should be given? Q: What do you expect to find at 13.00?