Download
1 / 1

E N D
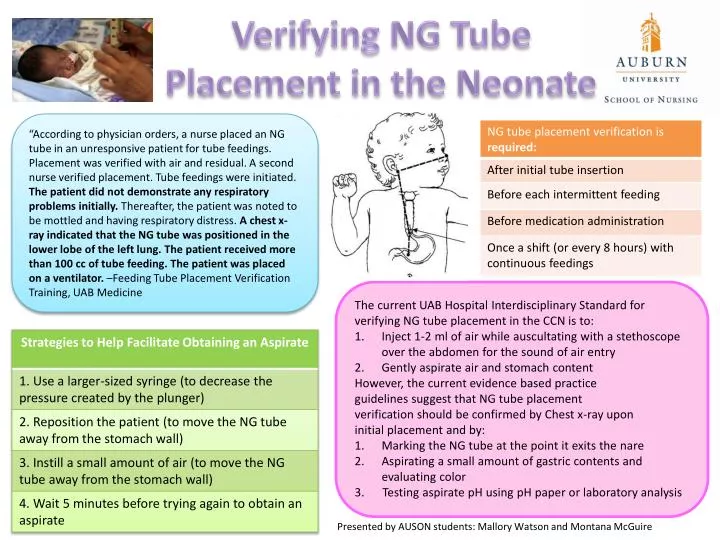
“According to physician orders, a nurse placed an NG tube in an unresponsive patient for tube feedings. Placement was verified with air and residual. A second nurse verified placement. Tube feedings were initiated. The patient did not demonstrate any respiratory problems initially. Thereafter, the patient was noted to be mottled and having respiratory distress. A chest x-ray indicated that the NG tube was positioned in the lower lobe of the left lung. The patient received more than 100 cc of tube feeding. The patient was placed on a ventilator. –Feeding Tube Placement Verification Training, UAB Medicine Verifying NG Tube Placement in the Neonate The current UAB Hospital Interdisciplinary Standard for verifying NG tube placement in the CCN is to: Inject 1-2 ml of air while auscultating with a stethoscope over the abdomen for the sound of air entry Gently aspirate air and stomach content However, the current evidence based practice guidelines suggest that NG tube placement verification should be confirmed by Chest x-ray upon initial placement and by: Marking the NG tube at the point it exits the nare Aspirating a small amount of gastric contents and evaluating color 3. Testing aspirate pH using pH paper or laboratory analysis Presented by AUSON students: Mallory Watson and Montana McGuire