Download
1 / 60
710 likes | 1.83k Views
Hepatic Physiology & Assessment and interpretation of liver function tests. Dr. M Sabra. Liver is the largest internal organ & largest gland in the human body.

E N D
Hepatic Physiology&Assessment and interpretation of liver function tests Dr. M Sabra
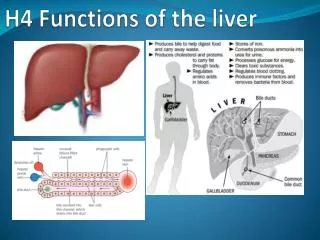
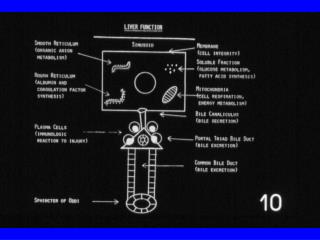
Liver is the largest internal organ & largest gland in the human body. • Liver is at the epicenter of intermediary metabolism , performs versatile & massive biochemical pathways and destroys bacteria, inactivate antigens, detoxify harmful chemicals. • Dual blood supply: Portal vein = 75% of HBF (55% of 02) , Hepatic artery = 25% of HBF (45% of 02) • Total hepatic blood flow = 25% of CO • Surgery and anesthesia impact hepatic function primarily due to their impact on hepatic blood flow and not primarily as a result of the medications or anesthetic technique utilized
Physiological functions of liver • Intermediary metabolism Carbohydrate metabolism Lipid metabolism Bile metabolsim Protein metabolism • Coagulation • Heme metabolism • Bilirubin metabolism • Xenobiotics metabolism ( a foreign chemical substance found within an oraganism , not normally naturally produced by organism. Eg drugs antibiotics • Storage • Endocrine functions • Immune & inflammatory response • Blood reservoir
Carbohydrate metabolism • Liver is an important homeostatic regulator of blood glucose. It can either produce glucose or store glucose • In fed state- polymerize glucose to glycogen • In unfed state- depolymerize glycogen to glucose • Glucose → hepatocytes → glycogen ↑ →glucose Lactate Glycerol aminoacids
Carbohydrate metabolism • Glycogen metabolism • Regulation – 2 rate limiting enzymes • Glycogen synthase- synthesis of glycogen from monomers of UDP glucose. • Glycogen phosphorylase- clevage of glycogen to glucose-1-phosphate.
Carbohydrate metabolism Gluconeogenesis • Liver glycogen stores depleted - hepatic gluconeogenesis to replenish blood glucose. • Substrates- - lactate - glycerol from hydrolysis of triglycerides - gluconeogenic amino acid , alanine , glutamine
Hormonal regulation of carbohydrate metabolism Glycogenesis Glycogenolysis Glucose 6-PO4 + + • Insulin • Glucagon • Epinephrine + B. Glucose B. Glucose
Blood glucose regulation within a narrow limit (70-100 mg/dl) not affected in liver disease due to large reserve of hepatic function • Effects of anaesthesia on carbohydrate metabolism • Halothane • release of insulin • rate of glycogenolysis • Inhibition of gluconeogenic response • Isoflurane • Impaired insulin secretion
Lipid Metabolism • Oxidation of fatty acids • Fatty acids derived from plasma • Enter into mitochondria • oxidation: fatty acids AcetylCoA citric acid cycle • Regulators - Glucagon - activates - Insulin - inhibits
Synthesis of lipoproteins • One of the major functions of the liver • Major classes • VLDL (Very low density lipoproteins ) • LDL ( low density lipoproteins ) • HDL (High density lipoproteins)
VLDL • Acute or chronic liver disease – ability to produce VLDL is markedly compromised • Liver VLDLs are associated with an important class of proteins, the apo B protein • Apo B100 - important for hepatic secretion of VLDL. • Decreased in ABETALIPOPROTEINEMIA • LDLs and HDLs • Liver produces them in a small amount
Production of ketone bodies • Most organs except the liver- use ketone bodies as fuel • Ketone bodies – acetoacetic acid, acetone, hydroxybutyrate • Their formation by the liver is normal and physiologically important, e.g. • Fasting rapid depletion of glycogen stores in the liver shortage of substrates for citric acid cycle • AcetylCoA formed from oxidation ketone bodies • Ketosis - conc. of ketone bodies in blood • Starvation • DM • After high fat diet
Synthesis of cholesterol • Important role in cholesterol homeostasis • Liver cholesterol has both exogenous and endogenous source • Uses of hepatic cholesterol • Formation of bile acids- conjugated with other substances to form cholic acid. • Synthesis of VLDLs
Bile metabolism & enterohepatic circulation • Bile salts are end products of cholesterol synthesis • Daily production – 600- 800 ml/d • Functions- - activate lipase - promote micelle formation - intestinal uptake of fat soluble vitamins, cholesterol & lipids - facilitate excretion of xenobiotics, lipophillic substances, bilirubin, amphipathic steroid hormone derivative
Bile salts undergo enterohepatic circulation (20-30 times/day) intrahepatic bile duct ↓ common hepatic duct cystic duct CBD ↓ ↓ gall bladdersmall intestine ( terminal ileum) • Clinical implication • Opioids can induce spasm of bile duct & spinter of oddi • Reversed by – glucagon, opioid antagonists ( naloxone), smooth muscle relaxant (NTG), antimuscarinic drugs( atropine), volatile anaesthetics.
Protein and amino acid metabolism • Deamination of amino acids • Required before they can be used for energy or before they can be converted into carbohydrates or fats • Formation of urea for removal of ammonia from the body fluids • Production of proteins and peptides.
Krebs- Hanseleit cycle Major pathway for removing NH3 & other nitrogenous wastes from body Captures nitrogen in form of urea. Failing liver- BUN remain low - ammonia accumulates in liver ↓ Hepatic encephalopathy
Proteins & peptides Albumin • Most abundant protein • Normal plasma conc- 3 - 5 g% • Daily production -12-15 g/d • Plasma half life – 15-20 days • Functions – • maintains plasma oncotic pressure (80% by albumin) • binds ions, bilirubin, hormones & drugs • Hypoalbuminemia – Colloid oncotic pressure edema
ᾳ- feto protein • Resembles albumin genetically & functionally • Formation sites- yolksac, hepatocytes, enterocytes • Fetal & neonatal life- major determinant of plasma oncotic pressure • 1 year of age- albumin largely replaces AFP • ↑ ↑ AFP- HCC
Fibrinogen • Synthesized exclusively by hepatocytes • Plasma fibrinogen – 100-700 mg/dl • Functions – polymerizes into long fibrin threads by the action of thrombin formation of clot
Haptoglobins • Forms stable complexes with free Hb prevents loss of iron through urinary excretion, protects kidney from damage • Ceruloplasmin – binds with copper and helps in its transport and storage • Wilson’s disease • Deficiency of ceruloplasmin free Cu2+ in circulation deposited in brain and liver
Coagulation • Synthesize most of the procoagulants except- • factor III ( tissue thromboplastin) • Factor IV ( calcium) • Factor VIII ( von Willebrand factor ) • Produce protein regulators of coagulation & fibrinolytic pathways • Protein C, protein S ( protein C – inactivate F VIIIa- Va complex) • protein Z ( degradation of Factor Xa ) • plasminogen activator inhibitor (PAI) ( inhibits tissue plasminogen activators to convert plasminogen to plasmin ) • antithrombin III
Liver as a Storage Organ • Vitamin A • Important role in the uptake, storage and maintenance of vitamin A levels by mobilizing its vitamin A store • Vitamin K • Vitamin K dependent factors II, VII, IX, X • Absorption of Vit K depends on normal fat absorption: any mal-absorption of lipid vitamin K deficiency • Storage in liver- limited hypoprothrombinemia can develop within a few weeks. • Treatment – • FFP • Antidote- parenteral vit K
Vitamin K cofactor & ỳ- carboxylation • Factor II, VII., IX, X , protein C & S- undergo Vit K dependent post translational modifications • Enables procoagulants to form complexes with calcium or other divalent cations for participation in the clotting cascade. • Clinical implication Warfarin inhibits vit K epoxide reductase ↓ traps Vit K in epoxide form ↓ Inhibits y- carboxylation • T/T- Enteral / parenteral Vit K. shuts
Storage & Homeostasis of Iron • Major site of synthesis of proteins (Transferrin, Ferritin) involved in iron transport & metabolism. • Heme metabolism Clinical implication • Porphyrias • Acute Intermittent Porphyria – commonest • Defects in the heme pathway- accumulation of porphyrinogens • Trigger substances- barbiturates, sex hormones, glucocorticoides, cigarette smoke, CYP inducers.
Bilirubin Metabolism • Main source of bilirubin is heme metabolism • Daily production- 300mg • 80 % derived from senescent erythrocytes by macrophages in RE system. • Heme ↓ ( heme oxygenase + o2 ) biliverdin IX + CO + free divalent iron ↓ ( biliverdin reductase) bilirubin
Plasma Fragile RBCs BILIRUBIN METABOLISM RE System unconjugated bilirubin (protein – bound) Liver Urobilinogen Kidneys Liver Conjugated bilirubin Absorbed Urobilinogen Urobilin Urine Bacterial action Oxidation Urobilinogen Stercobilinogen Stercobilin Intestinal Contents Oxidation
CO produced has many physiological roles • Vasodilation ( regulation of vascular tone) • Platelet aggregation • Vascular myocyte proliferation • Neurotransmitter release • Cytoprotective , antiapoptotic, antioxidant effects • Biliverdin – confers protection from oxidative effects • rapidly converts to bilirubin
Metabolism of Drugs (Xenobiotics) Factor affecting drug metabolism: microsomal enzyme system route of administration liver blood flow competitive inhibition • Phase-I reactions • Alter the parent drug by inserting or unmasking a polar group • Converts drugs to more polar compounds • Reactions – oxidations, reduction, hydrolysis • Cytochrome P450 – substrate binding site, located in the endoplasmic reticulum • Drugs– barbiturates, benzodiazepines, halogenated volatile anaesthetics, pethidine etc.
Phase-II reactions • Creates conjugates of parent compound or its metabolite with endogenous hydrophilic substrate • Reactions Glucoronidation Sulphation Methylation Acetylation • Glucoronidation • Most common type • Hepatic microsomal enzyme, UDPglucuronyl transferase mediates the transfer of glucoronic acid from UDP glucuronic acid to the functional group on the xenobiotics • Drug handled by phase-II – morphine, propofol, thiopentone (initially oxidized subsequently conjugated)
Phase-I reaction enzymes – more susceptible to destruction in cirrhosis • Phase-II reactions enzymes – more resistant, function even in advanced liver disease • Phase-III reactions • Involves ATP-binding cassette transport proteins (ABC) • These proteins use the energy of ATP hydrolysis to drive molecular transport • Dysfunction of ABC proteins hinders flow of bile predisposing to drug accumulation and cholestatic liver injury
Microsomal enzyme induction • Anticonvulsants, rifampicin, isoniazid, glucocorticoids, chronic alcohol consumption Consequences of enzyme induction • duration of action of drugs that are inactivated by metabolism • intensity of action of drugs that are activated by metabolism
Endocrine functions • Liver can modify or amplify hormone action • Metabolic conversion of Vitamin D to form 25(OH)D • 25(OH)D 1,25(OH)2D in kidney • Peripheral conversion of T4 to T3 • Pseudocholinesterase • Hydrolysis of succinylcholine • Plasma t½ - 14 days • Severe liver disease duration of action of succinylcholine
Insulin-like growth factors or somatomedins – growth hormone like action • Important role in cartilage function by promoting uptake of sulphate and synthesis of collagen • Removes circulating hormones • Insulin, glucagon, growth hormone, gastrointestinal hormones, e.g. gastrin
Blood reservoir • Liver is an expandable organ • 10 -15 % of total blood volume can be sequestered and quickly released after sympathetic stimulation . • Immune & inflammatory responses • kuffer cells protect against foreign intrutions, degrade toxins, process antigens, and phagocytose bacteria. • Induce & intensify inflammation by recruiting neutrophils • Release proinflammatory mediators
Liver Function Tests • Uses • To detect the presence of liver disease • To distinguish among different type of liver disorders • To guage the extent of known liver damage • To follow the response to treatment • Shortcomings of LFTs Can be normal in pts with serious liver disease and abnormal in pts with diseases that do not affect the liver Only categorises into hepatocellular or cholestatic
Classification of LFTs • Tests based on detoxification and excretory functions • Serum bilirubin • Breakdown product of porphyrin ring of heme containing proteins • 2 fractions - conjugated (direct – 30%) unconjugated (indirect – 70%) • Normal total serum bilirubin 1 mg/dl • in unconjugated fraction is rarely due to liver disease
Fractionate bilirubin >15% direct <15% direct Dubin Johnson syndr Rotor’s syndr Evaluation for hemolysis -ve +ve Crigler-Najjar syndr Gilbert’s syndr Hemolysis No further evaluation required
Urine bilirubin • Any bilirubin found in urine is conjugated, therefore bilrubinuria implies presence of liver disease • Blood ammonia • Detection of encephalopathy, monitoring hepatic synthetic function • Very poor predictor: presence/ degree of acute encephalopathy • Serum enzymes • No known function in serum • ed level- rate of entrance into serum from damaged liver cells
Enzymes categories • Enzymes that reflect damage to hepatocytes • Enzymes that reflect cholestasis • Enzymes that reflect damage to hepatocytes • Aminotransferases • Aspartate aminotransferase (AST or SGOT): Liver, cardiac muscle, skeletal muscle, kidneys, brain, pancreas, etc. • Alanine aminotransferase (ALT or SGPT): 1° in liver • Sensitive indicators of liver cell injury • Normal levels <35-45 IU/L
in aminotransferases • Mild - <250 IU/l • Any pathologic process that causes hepatocellular injury, e.g. hepatic steatosis, alcohol or drug induced liver disease, chronic viral hepatitis, cirrhosis, hemachromatosis • Moderate – 250-1000 IU/l • Disorder that produces hepatocellular necrosis • e.g. Acute viral hepatitis, drug induced hepatitis, exacerbation of chronic hepatitis (alcoholic) • Large - >1000 IU/l • Viral or drug induced liver damage superimposed on ALD, autoimmune hepatitis
AST/ ALT not ↑ in purely obstructive disorder except Acute biliary obstruction caused by passage of gallstones to CBD • Extreme - >2000 IU/l • Massive hepatic necrosis, usually from drugs (acetaminophan), halothane hepatitis, toxins, ischemic hepatitis (shock liver), acute viral hepatitis • AST/ALT ratio – DERITIS QUOTIENT • Normal - 1 or slightly > 1 • <1 – non-alcoholic steatosis or hepatitis without cirrhosis • 2-4 – ALD • >4 – Wilsonian hepatitis
LDH • Normal level -25-100 IU/L • Massive but transient - Ischemic hepatitis • Massive, sustained - Malignant infiltration of liver • Other causes of LDH • Hemolysis • Renal infarction • Acute stroke • Myocardial damage • Skeletal muscle injury
Glutathione S transferase • Relatively sensitive and specific test for detecting drug-induced hepatocellular injury • Plasma t½ 90 min, rapidly released into the circulation following hepatocellular injury • Plasma GST ( isoenzyme B ) – reveal time course of hepatocellular injury from onset to resolution • GST – located in the centrilobular region (zone 3), where hepatocytes are most susceptible to injuries from hypoxia and reactive drug metabolism
Bromosulphathein excretion test • BSP dye- same mechanism as bilirubin -binding -conjugation -excretion • BSP – i/v – 45 mins- levels in venous blood • Normally- <5%. • Slightly higher in old age • Sensitive test to detect mild impairement of liver
Enzymes reflecting cholestasis • Alkaline phosphatase- present in cells of the bile duct • Isoenzymes- bone , liver, intestine, placenta , kidney , leukocytes. • Normal levels- 42-122 IU/L - 3-13 KA units/dl
in serum ALP in an apparently healthy pt. • Fractionate the ALP to identify source of isoenzyme • ALP from different tissues differ in susceptibility inactivation by heat • Measure - 5' NT, GGT
5' NT • Sensitive and specific for hepatobiliary disorders (HBD) • Normal pregnancy, bone growth and bone diseases do not affect 5' NT • In pts with HBD, changes in ALP are usually followed by similar changes in 5' NT • GGT • Inducible microsomal enzyme. N levels – 5- 40 IU/L. • Less specific than 5' NT as a marker for HBD • Unlike 5' NT, GGT may be released from many sites beside the hepatobiliary tree • Bone – important source of ALP, has little GGT thus GGT useful for differentiating hepatic & osseous sources of ALP
Tests for bio-synthetic function of the liver • Estimation of plasma proteins • Tests for reversal of A:G ratio • Tests for coagulability of blood
Serum albumin • S. albumin <3 g/dl suspect chronic liver disease • Hypoalbuminemia – not specific for liver disease • Protein malnutrition of any cause • Protein losing enteropathies • Nephrotic syndrome • Chronic infections • Burns • Reversal of A : G ratio chronic liver dysfunction.