Download
1 / 42
420 likes | 560 Views
Helping HR & Line Managers to Understand & Manage Depression VTA HR Conference, May 2006 Clare Shann Program Manager beyondblue National Workplace Program. Depression is a treatable condition. People can fully recover, or manage their illness, and live fulfilling and successful lives.

E N D
Helping HR & Line Managers to Understand & Manage DepressionVTA HR Conference, May 2006Clare ShannProgram Managerbeyondblue National Workplace Program
Depression is a treatable condition. People can fully recover, or manage their illness, and live fulfilling and successful lives.
In order to achieve recovery we need to: -Understand what depression is -Know how to recognise it -Respond appropriately so effective treatments are used
What constitutes a ‘case’ of depression? • Depression is not just feeling sad or down • It is a clinical state • not just low mood but a serious illness • causes significant distress • Impairs their ability to manage their life
The diagnosis of depression • More than two weeks of persistent depressed mood and/or loss of interest or pleasure PLUS symptoms in at least 3 of the following categories Thoughts Negative thinking: “ hopeless, helpless and worthless” Suicidal thoughts Feelings Overwhelmed Unhappy Guilty Indecisive Disappointed No confidence Irritable Physical Tiredness Appetite/weight change Headaches Disturbed sleep Sick/run down Behavioural Withdrawal Unproductive Alcohol/sedatives Stop enjoyable activities Concentration difficulties
What is depression? • Depression is an illness • Like asthma, diabetes, epilepsy • May go on for weeks or months if left untreated • May be caused by a complex web of factors
Do we need to isolate the cause for each person? • There is not always a specific incident • Often we can’t identify, control or change what caused depression • Effective treatment can be solution focused
How common is depression?(Derived from Australian National Household Survey 1999)
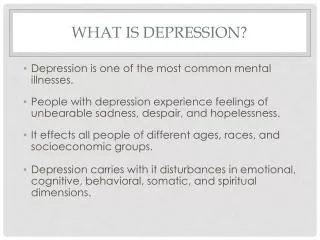
How common is depression in the Australian community? N= 10 600 Twelve-month prevalence of mental disorders in Australian adults MALES FEMALES % Population % Population estimate estimate Any depressive disorder 4.2 275,300 7.4 503,300 Any anxiety disorder 7.1 470,400 12.0 829,600 Any substance use disorder 11.1 734,300 4.5 307,500 Any mental disorder 17.4 1,151,600 18.0 1,231,500 Source: Andrews G, Hall W, Teesson M, Henderson S. The mental health of Australians. Mental Health Branch, Commonwealth Department of Health and Aged Care, 1999.
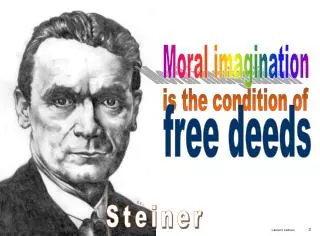
Depression across the lifespan Prevalence of depression by age and sex Source: Andrews G, Hall W, Teesson M, Henderson S. The mental health of Australians. Mental Health Branch, Commonwealth Department of Health and Aged Care, 1999.
Prevalence • Over 800,000 Australians each year suffer from a depressive illness • Depression affects 1 in 5 people in their adult lifetime • 1 in 4 women, and • 1 in 6 men will suffer from depression at some time in their adult life 1 in 5 in your community, and your organisation
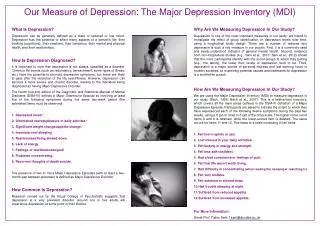
What does depression cost the community? The 10 leading causes of disease burden (DALYs) in Australia DISEASE % OF DALYs† 1. Ischaemic heart disease 12.4 2. Stroke 5.4 3. Chronic obstructive pulmonary disease 3.7 4. Depression 3.7 5. Lung cancer 3.6 6. Dementia 3.5 7. Diabetes mellitus 3.0 8. Colorectal cancer 2.7 9. Asthma 2.6 10. Osteoarthritis 2.2 † Disability-adjusted life year (DALY) = is a measure of the years of ‘healthy’ life lost due to illness or injury (one DALY is one lost year of ‘healthy’ life). Source: Mathers C, Vos T, Stevenson C. The burden of disease and injury in Australia. Australian Institute of Health and Welfare (Catalogue number PHE 17). Canberra: AIHW; 1999.
What are effective treatmentsfor depression? • Psychological – eg. Cognitive-behaviour therapy, interpersonal therapy • Medical – eg. Antidepressant medication, electroconvulsive therapy (for severe depression only) • Lifestyle – eg. Physical activity, light therapy (for seasonal winter depression) The most important thing is to find a treatment that works for the individual ! Jorm et al 2001
Seeking treatment for depression • Of 800,000 Australians (population estimate) Only 38% access any mental health intervention 62% do not get any mental health intervention 75% dealt with in primary care ONLY 15% received any evidence-based intervention
beyondblue established • beyondblue: the national depression initiative • Similar structure to the Cancer Council/National Heart Foundation • Does not provide clinical services • Education, health policy reform, research
beyondblue • Funded by Commonwealth & all State & Territory Governments • Funded initially for 5 years, now funded for further 5 year term • Launched March 2000 (chairman Hon Jeff Kennett) • National body based in Melbourne (small team of 20)
beyondblue’sWorkplace Program Depression: it’s our problem?
Rationale for workplace program • Impact of Depression on work • Depression reduces a person’s ability to function in all aspects of their life, including work, social and home life • Depression results in… • Over six million working days lost each year • half a million full working days lost every month, • more than 12 million days of reduced productivity in a year Source: Andrews G, Hall W, Teesson M, Henderson S. The mental health of Australians. Mental Health Branch, Commonwealth Department of Health and Aged Care, 1999.
It is estimated that each employee with untreated depression will cost their organisation $9,660 per year (Caleo & Hilton, Q’land Centre for Mental Health Research 2004) • Majority of cost due to lost productivity while at work with days off work due to illness also contributing (cost does not include losses due to WorkCover or insurance claims, PT or casual employees, staff attrition or critical incidents) • Psychological injury represents around 7% of claims but 27% of total claim costs(Better health at work Conference, Comcare & HSA 2005)
Discrimination in the workplace • Makes it hard for people to come forward • People feel they will be branded with it forever • ‘weakness versus illness’ issue “Now I am unlikely to be considered for promotion – I am considered to be inadequate – even when I’m well!” “I was asked to chart the days that I would be taking off sick over the rest of the year, and when I couldn’t do that I ended up losing my job.” “I finally plucked up the courage to tell my manager that I suffer from depression, and I was given filing to do.”
Attitudes which may impact on the workplace… • 36% believe that people with depression in positions of high responsibility should quit their jobs • 36% believe that people with severe depression should pull themselves together Highet et al, 2001, 2002, 2005 Many managers do not know how to deal with depression.
About the beyondblueworkplace program:EDUCATION-signs and symptoms-effective treatments-accessing helpATTITUDES AND BEHAVIOURS-correcting misconceptions-reducing stigma-increasing confidence and willingness to interveneSKILLS DEVELOPMENT-identifying those needing assistance-responding appropriately
Useful strategies – reinforced through use of case studies • Approach, engage – don’t isolate further • Talk to them • Reassure valued/not blame • Realise there does not have to be a cause • Share personal experiences/health agencies/EAP • Encourage professional help • Encourage social support/interaction • Follow-up
website Supporting resources/materials- fact sheets & information cards for all participants- posters for display in workplace(reinforces key messages in training)- beyondblue & Ybblue website (GP list downloadable resources)-link from your website to ours-information for your intranet-links to on-line treatment- mental health policy in development
To access Consenting Practitioners’ List Click on State Currently 750 GPs with BOIMH training
Does implementation of the program lead to behaviour change?
Evaluation of Workplace Program • Baseline surveys • Pre and post workshop (& follow-up) • Pilot – integrate key messages/issues into training • Workplace Training vs Train the Trainer • Linking with EAP – assess rates of access • Evaluation report provided to organisation
Management Feedback “I thought that giving time off work would be helpful, I never considered how this would increase the isolation and make it harder (for my employer) to return to work” Manager
Participant feedback …..Now on medication, my life has improved 100%. Not only at home but in my approach to work and my ability to cope with stress. This has resulted in my being more productive This is a sincere thank you, for drawing my attention to the problem and for what has been a significant change in my life and that of my family. Employee
One ‘host’ per table, welcomes guests and holds threads of the discussion together to report back to larger group • 4 ‘rounds’ of discussion • ‘Guests’ move around tables each round • Try to work with as many different people as possible • Last round: return to original table, work with host to agree on what host will present (informally) to the larger group
Role of ‘Host’ • Remind people to jot down key ideas • Remain at the table when others leave and welcome ‘guests’ from other tables • BRIEFLY share key insights from the prior conversation so others can build on those • Be prepared to share your table discussions with the larger group
Discussion topics Round 1: PASTHas anything been done in the past to manage mental illness in your workplace in a systematic way? If so, what has gone well? What hasn’t? What were the consequences? Round 2: PRESENTWhat is the current situation in terms of the management of mental health/illness in your organisation? What are your current challenges in this area? How can you address these challenges? What can the VTA do to support you?
Discussion topics cont… Round 3: What obstacles do you potentially see in the future in managing mental health in the workplace? How might you overcome these? What can the VTA do to support you? Round 4: Decide, as a group, what your host will present back to the larger group to address the big question: In what ways can your organisation better understand and manage mental health/illness in the workplace and how can the VTA assist with this?
Remember • The table host must encourage guests to: • Brainstorm & discuss questions • Build on previous conversations • In the final round, there must be agreement at the table on what the host will present back to the group • Host from each table presents a brief & informal report on the discussion
Questions and comments about the program: Clare Shann (Program Manager) & Michael O’Hanlon (Business Manager) workplace@beyondblue.org.au Phone: (03) 9810 6100 www.beyondblue.org.au