Download
1 / 42
420 likes | 544 Views
Tennessee Connections for Better Birth Outcomes: Working to Improve Maternal and Infant Health. Melanie Lutenbacher, PhD, MSN, APRN, FAAN Infant Mortality Best Practices Forum August 31, 2011. Infant Mortality. complex phenomenon societal issues lifestyle choices

E N D
Tennessee Connections for Better Birth Outcomes:Working to Improve Maternal and Infant Health Melanie Lutenbacher, PhD, MSN, APRN, FAAN Infant Mortality Best Practices Forum August 31, 2011
Infant Mortality • complex phenomenon • societal issues • lifestyle choices • biological factors indicator of overall maternal/child health
The Company We Keep… Infant Mortality Rates
Why Do Our Babies Die? • congenital malformations& chromosomal abnormalities • short gestation and low birth weight • sudden infant death (SIDS) • newborn affected by maternal complications of pregnancy • unintentional injuries Source: National Vital Statistics Report 2006
Acute Morbidity by Gestational Age Among Surviving Infants Results of a community-based evaluation of 8523 deliveries, 1997–1998, Shelby County, Tennessee Mercer BM ObstetGynecol 2003;101:178 –93.
Escalating Hospital Costs with Decreasing Gestational Age (Phibbs and Schmitt, 2006 Journal of Early Human Development)
One Premature Birth Significantly Increases the Likelihood for Recurrence Adams, 2000
Synergistic Relationships Best Practice Science Translational Research Evidence Based
Preterm Birth Prevention • we don’t have all the answers… • BUT, we know some of the factors that contribute to preterm births… • AND…we have some promising interventions.
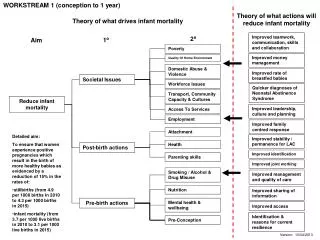
Modify Maternal Risk Factors • Adequate health coverage • Available resources • Multiple methods of service delivery • *clinic *group *texting • *home visit *telephone *internet PTB Infant Mortality • Stress • Infections • Domestic violence • Smoking • Substance abuse • Nutrition • Dental Health • Interpregnancy intervals System of Care • Pre-conception / inter-conception care • Early prenatal care • Enhanced support through pregnancy
Tennessee Connections for Better Birth Outcomes • Translated existing evidence intointerventions • Targeted modifiable risk factors in pregnant women • With history of at least one preterm birth Funded by BCBS TN Health Foundation With support from: VU Clinical Translational Science Award grant UL1 RR024975-01 from NCRR/NIH VU School of Nursing Center for Research Development and Scholarship
BBO Research Team • Melanie Lutenbacher, PhD, MSN, APRN, FAAN* • Patricia Temple Gabbe, MD, MPH, Pediatrician*+ • William F. Walsh, MD, Neonatologist • Etoi Garrison, MD, High Risk Obstetrician • Lavenia Carpenter, MD, High Risk Obstetrician • Mary S. Dietrich, PhD, Biostatistician * • Sharon Karp, PhD, MSN, CPNP* • Deborah Narrigan, MSN, CNM • Jennifer Murray, PhD (c) * Appointments at Vanderbilt University Schools of Nursing and Medicine *+ Appointment at Ohio State University Schools of Nursing and Medicine
Study Goals • improve maternal health in women with a history of at least one prior PTB via • evaluation of the feasibility and efficacy of a system of care to reduce preterm births & the associated health care costs
BBO Study Design Observational Group (decline main study) Random Assignment
Who could participate? • Confirmed pregnancy • 18 – 40 years of age • History of preterm birth (Live birth > 20wks and <37wks) • Reside in Davidson or surrounding county (up to 90 miles) • < 24 wks gestation at enrollment • Receive prenatal care at VUMC • Willing to accept nurse home visits & be randomly assigned • Speak & understand English
BBO Before Delivery Collaborative Prenatal Care • nurse midwife conducted home visits to augment standard care • intervention focused on: • establishing supportive relationship • reinforcing clinical care including 17-P therapy as appropriate • monitoring maternal condition • reducing the risk of stress, depression, smoking, poor nutrition, alcohol/substance abuse/misuse, domestic issues • defining reproductive life plan • facilitating preparation for breastfeeding
BBO After Delivery for 18 months • first post-partum visit within 48 hours of birth, with hand-off to maternal/child nurse for 18 months of care • home intervention focused on: • establishing supportive relationship • continuing to address risks identified prenatally • supporting reproductive life plan • monitoring infant conditions including continuity with medical home
Data Sources • scheduled interviews (standardized measures) • medical center charge records • medical/hospital records (maternal & infant) • study records (e.g., screening logs, travel records, clinical forms) • follow up surveys (participants, providers)
Intervention Fidelity • visit guidelines r/t to each risk factor • nurse interventionist training • 24/7 clinical and study protocol backup • study specific ‘clinical’ visit forms • pocket ‘cue’ cards • study specific charting template in VU OB EMR • case reviews • direct observation of home visits • review of completed documents
Key Risk Factors Assessed • # prior PTBs • African American race • pregravid BMI • smoked • reported domestic violence • # medical conditions • # prenatal hospitalizations Level of: • depressive symptoms • maternal stressors • social support • sense of personal mastery & control
Women with Similar Clusters of Risk Factors • exploratory method of “classifying” cases on multiple dimensions • helpful for seeing patterns in complex data • generates groups of cases with similar patterns or characteristics into a cluster • separates groups with discrepant or inconsistent patterns • defined groups can be used for further analyses
Cluster 1 (N = 30) • Compared to other clusters: • Lowest % smoke • Healthy, ‘normal’ BMI • Lowest in stress & depressive symptoms • Higher sense of personal control Cluster
Cluster 2 (N = 59) • Compared to other clusters: • Higher % African American • Overweight • Have more medical conditions • including prenatal hospitalization • Higher stress, depressive • symptoms, reports of DV Cluster
Cluster 3 (N = 33) • Compared to other clusters: • Healthy, ‘normal’ BMI • Lower stress & depressive symptoms • Lower sense of personal control Cluster
Cluster 4 (N = 36) • Compared to other clusters: • Higher % smoke • “Normal” BMI; healthy • > number prior preterm births • High social support and • sense of personal control Cluster
Cluster 5 (N = 30) • Compared to other clusters: • “Normal” to low BMI • Higher stress & depressive • symptoms levels • Higher social support and • sense of personal control Cluster
Depressive Symptoms • At study enrollment, 28% of women had high depressive symptoms • At 48 hours postpartum, after controlling for baseline depressive symptoms: women in the intervention group had a greater reduction in depressive symptoms than those in the control group
Where Do We Go From Here? • further examine women with specific clusters of risk factors • examine these clusters in relation to amount and focus of home visits • share lessons learned • refine intervention, study materials, and design • test
remember - prevention of infant mortality begins long before the baby arrives educate yourself, family members, friends & co-workers about risk factors for preterm birth use evidence to guide your efforts to promote healthy behaviors support adequate health care coverage & access get involved with efforts to prevent preterm births What Can You Do?