Download
1 / 35
350 likes | 456 Views
Evidence Based Guidelines at PHD related to Infectious Disease. Edward L. Goodman, MD. Outline. Standing Orders for Vaccinations The problem Evidence for guidelines Federal Guidelines Comprehensive Antimicrobial Management Program Evidence in the literature Components of Program

E N D
Evidence Based Guidelines at PHD related to Infectious Disease Edward L. Goodman, MD
Outline • Standing Orders for Vaccinations • The problem • Evidence for guidelines • Federal Guidelines • Comprehensive Antimicrobial Management Program • Evidence in the literature • Components of Program • Outcomes to date
Standing Orders for Influenza and Pneumonia Vaccine • Background • Interventions in the literature • Federal support • Implementation
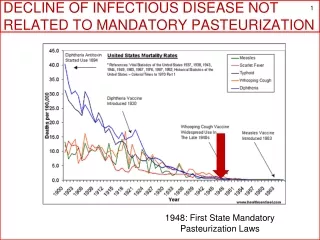
Background: http://www.cms.hhs.govhealthyaging/2a.asp • Influenza and pneumonia represent 5th leading cause of death in elderly • 20,000 to 40,000 influenza related deaths annually • 90% occur in those >65 years old • Influenza vaccine effective • Reduces hospitalizations by 27-57% • Reduces deaths by 27-30%
Underutilization • Influenza/pneumococcal vaccines are underutilized for persons >65 • Overall, 66%/35% • Nursing Homes 68%/38% • National Center for Health Statistics. Early release of selected estimates from the 2002 National Health Interview Surveys. http://www.cdc.gov/NCHS/about/major/nhis/released200209.
Cost effectiveness of Influenza vaccination. Leavenworth, G. The costly toll of vaccine-preventable disease. Business and Health 1995;(13)(3)16 • Minnesota health plan, three flu seasons • Vaccinated 45-58% of those >64 years • Lower hospitalization rates for flu, pneumonia, CHF • Average savings of $117 per vaccinated member
Standing Orders Improve Rates • Task Force on Community Preventive Services. Recommendationsregarding interventions to improve vaccination coverage in children,adolescents, and adults. Am J Prev Med 2000;18:92—140 • . Health Care Financing Administration. Evidence report andevidence-based recommendations: interventions that increase the utilizationof Medicare-funded preventive service for persons age 65 and older.Baltimore, Maryland: U.S. Department of Health and Human Services, HealthCare Financing Administration, October 1999; HCFA publication no.HCFA-02151. • Crouse BJ, Nichol K, Peterson DC, Grimm MB. Hospital-basedstrategies for improving influenza vaccination rates. J Fam Prac 1994;38:258--61. • Stevenson KB, McMahon JW, Harris J, Hilman JR, Helgerson SD.Increasing pneumococcal vaccination rates among residents of long-term-carefacilities: provider-based improvement strategies implemented by peer-revieworganizations in four western states. Infect Control Hosp Epidemiol2000;21:705--10.
Government Regulations to Promote Standing Orders • Centers for Medicare and Medicaid Services. Medicare and Medicaidprograms: conditions of participation: immunization standards for hospitals,long-term care facilities, and home health agencies. Washington, DC: U.S.Department of Health and Human Services, Centers for Medicare and MedicaidServices, 2002. Available athttp://www.cms.gov/providerupdate/regs/cms3160fc.pdf<http://www.cms.gov/providerupdate/regs/cms3160fc.pdf> . Centers for Medicare and Medicaid Services, Center for Medicaid andState Operations. Program memorandum: change in requirement for signedphysician's order for influenza and pneumonia vaccine. Washington, DC: U.S.Department of Health and Human Services, Centers for Medicare and MedicaidServices, 2002; publication no. S&C-03-02.
Rationale • Antibiotic use (appropriate or not) leads to microbial resistance • Resistance results in increased morbidity, mortality, and cost of healthcare • Appropriate antimicrobial stewardship will prevent or slow the emergence of resistance among organisms (Clinical Infectious Diseases 1997; 25:584-99.) • Antibiotics are used as “drugs of fear” • (Kunin et al.Annals 1973;79:555)
Antibiotic Misuse • Surveys reveal that: • 25 - 33% of hospitalized patients receive antibiotics (Arch Intern Med 1997;157:1689-1694) • 22 - 65% of antibiotic use in hospitalized patients is inappropriate (Infection Control 1985;6:226-230)
Changes in Resistance Rates at a University Hospital • A university hospital had an increase in multidrug-resistant K. pneum. • Physicians were educated about the association between ceftazidime use and MDR K. pneum. • Education occurred through grand rounds, attending rounds and consultations by ID physicians and clinical pharmacists. • Infect Control Hosp Epidemiol. 2000;21: 455-458.
Resistance Changes in a Community Hospital • Increase resistance among GNR with C-I beta-lactamases, staph and enterococcus • An antimicrobial task force was formed (ID physicians, pharmacists, microbiologists, and infection-control.) • Consultations were triggered by 3rd generation cephalosporins, carbapenems, and vancomycin. • Extended spectrum penicillins/beta-lactamase inhibitor and aminogycosides were encouraged. • Costs were reduced by $650,000/year. • Pharmacotherapy 1999;19(8 pt 2):129S-132S
Changes in Resistance at an Urban Teaching Hospital • Epidemic in the surgical ICU of bacteremia due to Acinetobacter sensitive only to imipenem • Prior-authorization from ID faculty for selected antibiotics (amikacin, aztreonam, ceftaz, cipro, imipenem, ticar/clav) was required. • Acquisition cost for antimicrobial drugs were reduced by $863,100/year. • Survival rates, LOS, and length of ICU stay were not impacted. • Clinical Infectious Diseases 1997;25:230-9.
Components of PHD Program • Intravenous (IV) to oral conversion for well absorbed (highly bioavailable) antimicrobials • Discontinuation of preoperative antibiotic prophylaxis at 24h • Restricted antibiotic therapy
Components of the Program 1 • IV to Oral Conversion for Highly Bioavailable Antimicrobials • Patient Criteria • Able to take oral medications and diet • No persistent nausea, vomiting, or diarrhea • No medical condition that could decrease drug absorption • IV to oral conversions became automatic on July 1, 2001 • Pharmacists consult with nurse about how well the patient is eating and taking medications
Components of the Program 2 • Discontinuation of Preoperative Surgical Prophylaxis at 24 Hours • Strong support in the medical literature • Undergoing a “clean” procedure • Open heart • Artificial joint insertion • Many others
Components of the Program 3a • Restricted Antimicrobial Therapy • Antimicrobial Criteria • High risk • High cost • High potential to select resistance • Drugs of “last resort”
Components of the Program 3b • Restricted AntimicrobialTherapy • Antimicrobials restricted to ID physicians • Quinupristin/Dalfopristin (Synercid®) • New Antifungal Agents • Antimicrobials restricted after 48 hours – require Infectious Disease consult to continue • Vancomycin • Imipenem/Meropenem • Cefepime • Ceftazidime • Linezolid
Results of CAMP • April 2001 inception and partial implementation • July 1, 2001 full implementation
Antimicrobial Program Interventions(April 3, 2001 - December 31, 2002) Table 1
Team Activities To Date Including 2003 • 30 - 60 antimicrobial orders screened daily • > 1400 antibiotic recommendations have been made since April 1, 2001 • Recommendations are communicated through notes on charts and phone calls • Overall acceptance rate is 79%