Download
1 / 68
1k likes | 2.61k Views
Aqueous Production and Intraocular Pressure. Aqueous Production. Sometimes less is more!. Introduction. The aqueous has two important ocular functions: By maintaining an optimal IOP it permits the proper optical performance of the eye

E N D
Aqueous Production Sometimes less is more!
Introduction • The aqueous has two important ocular functions: • By maintaining an optimal IOP it permits the proper optical performance of the eye • The flow of aqueous from the posterior chamber, through the pupil, into the anterior chamber provides nutritional support for the avascular structures it bathes • Normal production and drainage causes the aqueous to be replaced completely every 100 minutes • The aqueous is secreted by the nonpigemented epithelium (NPE) of the ciliary body—the pigmented epithelium (PE) also plays a role in its formation
Ciliary Anatomy Review • The ciliary body is divided into two zones: 1) the smooth pars plana and the pars plicata, which features 70-80 ciliary processes, radially arranged ridges, each about 1 mm high, 2 mm long, and 0.5 mm wide • The ciliary body is anchored to the scleral spur, which is about 1.5 mm posterior to the corneolimbal junction • Most of the ciliary body is smooth muscle arranged into longitudinal, radial, and circular bundles
Ciliary Anatomy Review • The supraciliary space is a potential space, which lies between the ciliary body and the sclera • Both the pars plana and the pars plicata are lined by a double layer of epithelial cells • The innermost epithelial layer (relative to the center of the eyeball) is nonpigmented and the outermost is pigmented • The cells in the two layers lie apex to apex, and their basal surfaces lie upon basement membranes they both secrete
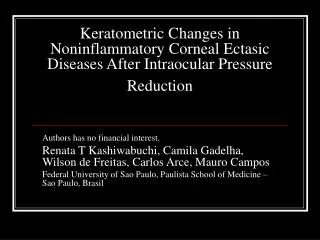
a - pigmented iris epithelium b – non pigmented ciliary epithelium c- basement membrane d – dense collagenous connective tissue. e – pigmented ciliary epithelium
Ciliary Processes • The ciliary body is supplied with blood via the anterior ciliary and long posterior ciliary arteries, which anastamose to form the major circle of the iris • Each ciliary process has a vascular core and are the most vascular structures in the eye • The arteries at the crests of the processes show focal constrictions that likely serve to regulate perfusion pressure and influence ultrafiltration • Blood flow in the processes is reduced by sympathetic stimulation or by adrenaline
Ciliary Processes • There is an extensive capillary system close to the basement membrane of the pigmented epithelium • The endothelial lining of these capillaries is fenestrated (30-100 nm) and is, therefore, highly permeable • Also, the endothelial cells do not tightly connect to one another and do not have anchoring or tight junctions
Ciliary Epithelium • The inner nonpigmented epithelial layer (NPE) is in direct contact with the aqueous humor, and the outer layer, the pigmented epithelial layer (PE), lies between the NPE and the ciliary stroma • The choroid’s Bruch’s membrane is continuous with the internal limiting membrane of the ciliary body and serves as a basement membrane for the PE • The PE is formed from the outer layer of the optic cup and so is continuous with the retinal pigment epithelium posteriorly and the anterior iris epithelium anteriorly (the epithelium of dilator muscle origin)
Ciliary Epithelium • The PE’s cells are cuboidal and contain many melanosomes and organelles, but not as many as the NPE • The NPE layer is formed from the inner layer of the optic cup and is continuous with the neural retina posteriorly and the posterior layer of the iris epithelium anteriorly • Its cells are columnar and contain a large amount of mitachondria and rough and smooth endoplasmic reticulum, both found in cells with a high metabolic rate
Ciliary Epithelium • The NPE cells have numerous basal enfoldings and convoluted lateral interdigitions—ciliarychannels run between the apices of the NPE and PE cells • Zonula occludens are found between the lateral walls of the NPE cells near their apices (close to the PE)—These junctions make the epithelium a “tight barrier” • Desmosomes are located between the lateral surfaces of the NPE cells and less frequently between the PE cells, and at the apices of the PE and NPE cells
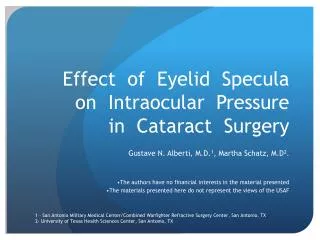
Posterior chamber Pump locations Tight junctions Ciliary Channels Ciliary stroma
Ciliary Epithelium • Gap junctions connect the walls of the PE cells and to a lesser extent those of the NPE • Gap junctions and puncta adherens are found at the interface between the PE and the NPE cells • The gap junctions electrically couple the PE and NPE cells and cause them to act as a syncytium, which is necessary to coordinate their roles in the secretion of aqueous
Blood-Aqueous Barrier • Erhlich (1885) and Goldmann (1913) showed that intravascular trypan blue stained all tissues in the body except the central nervous system • The mechanism responsible was named the blood-brain barrier, and there is a similar exclusion process in the eye, the blood-aqueous barrier • Consequently, many substances present in the blood plasma are not found in the aqueous humor • The most obvious difference is that only a fraction (about 1/300th) of the protein found in the plasma is found in the aqueous
Blood-Aqueous Barrier • This low protein level is essential in keeping the aqueous free from optical flare and scattering that would be caused by the large protein molecules • The tight junctions of the NPE are responsible for much of this barrier • After certain pathological conditions, plasma protein can leak into the aqueous creating a “plasmoid” or “secondary” aqueous • This abnormal aqueous can lead to an increase in IOP, probably due to large-protein drainage problems
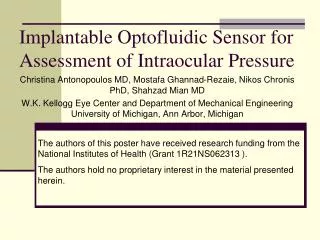
Posterior chamber Pump locations Tight junctions Ciliary Channels Ciliary stroma
Aqueous Humor Production • There are three possible ways that substances may cross an epithelial barrier: diffusion, ultrafiltration and active transport—active transport plays the major role in the secretion of aqueous • Active transport uses cellular energy to secrete solute against a concentration or electrical gradient • Diffusion of a solute (usually lipid-soluble) across a semipermeable membrane occurs along the concentration gradient • Ultrafiltration refers to the bulk flow of material assisted by a hydrostatic pressure (fluid pressure) head
Active Secretion • It was first thought that aqueous was formed by diffusion or ultrafiltration of fluid from the blood plasma • However, when metabolic-pump poisons are used, the IOP drops significantly to one-third its normal amount • It is now established fact that active transport is the most important mechanism in the formation of aqueous
Active Secretion • The specific transport system is the membrane-bound enzyme complex, sodium-potassium adenosine triphosphate (Na+/K+ ATPase) • These pumps are found in the NPE, mostly along the lateral cellular interdigitations • Poisoning of these pumps with oubain greatly decreases aqueous production • It is most likely that Na+ is the transported ion, although the amount of Cl- and HCO3- is not known
Active Secretion • Given that the Na+/K+ ATPaseis in highest concentration along the lateral cellular interdigitations, it’s likely that Na+ is actively transported into the proximal end (closest to the PE) of the lateral channel between the NPE cells • This ionic transport renders the fluid in this proximal region hypertonic, which results in an osmotic flux of water into the intercellular channel • The concentration of solute decreases as the fluid nears the posterior chamber, and this slightly hypertonic fluid is new aqueous
Active Secretion • Other enzyme systems have been identified in the NPE, including adenylate cyclase, an enzyme that regulates the conversion of ATP to cAMP, and also carbonic anhydrase, which promotes the production of bicarbonate
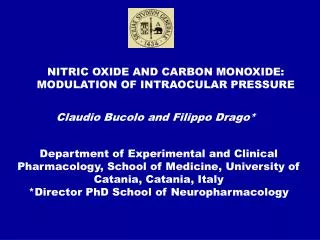
Tight junctions Posterior chamber PE
Ultrafiltration • The net hydrostatic force that moves aqueous from the blood plasma to aqueous is quite small, due to the resistance of tissue oncotic pressure • Given that the inhibition of Na+/K+ ATPase by oubain decreases aqueous production by about 70%, ultrafiltration is not a major factor in the production of aqueous • The capillary pressure needed to drive effective ultrafiltration is much higher that that which exists
Variations in Aqueous Production • Aqueous flow is used as an indicator of aqueous production and is assessed with the use of fluorescein—the amount of fluorescence decrease with time is measured • This technique underestimates aqueous production because some aqueous is absorbed into the vitreous, lens, and iris • When a person is awake the aqueous flow is about double that of when the person is asleep—this is possibly due to hormone level change
Variations in Aqueous Production • Aqueous production decreases steadily with age, about a 3% decrease per decade • The age decrease may be due to changes in the ciliary epithelium, which include cell loss, or due to age-related hormone level change
Control of Aqueous Production • There is some mechanism, neural or hormonal, that regulates the production of aqueous and so controls the eye’s IOP • Adenylate cyclase may play a role, but the nature of the regulation of aqueous production is not yet known
Carbonic Anhydrase Inhibition • Acetazolamide, which inhibits carbonic anhydrase and reduces the production of HCO3-, decreases IOP through a reduction in aqueous production • Acetazolamide causes a reduction in Cl- aqueous concentration and decreases the rate of HCO3- and Na+ transport, which likely means that these two ions are linked
Chemical Composition of the Aqueous • Osmolarity:There is little osmotic difference between aqueous and blood plasma, and none between the aqueous of the anterior and posterior chambers • Electrolytes: There are many differences in the concentration of electrolytes between the aqueous and blood plasma • Glucose: The aqueous concentration of glucose is about 80% that of the plasma and likely enters it by simple diffusion
Chemical Composition of the Aqueous • Lactate: Lactic acid is found in higher concentration in the aqueous than in the blood plasma; the metabolic activity of the lens, cornea, and ciliary body all dump lactic acid into the aqueous • Ascorbate: The high level of ascorbate found in the aqueous is puzzling. It seems to be actively secreted by a transport mechanism. Ascorbate serves as an antioxidant, may help regulate the mucopolysaccharides in the trabecular meshwork, or may absorb UV
Chemical Composition of the Aqueous • Amino Acids: There is a significant difference between the concentration of some amino acids in the aqueous and the blood plasma. There may be as many as six transport mechanisms for various amino acids, though specific evidence is lacking • Proteins: The blood-aqueous barrier causes the aqueous level of protein to be less than 1% of that of the plasma concentration, with the lower molecular weight proteins being more common in the aqueous. • Lipids: The blood-aqueous barrier restricts phospholipids to a fraction of their plasma concentrations
Pathological Changes in the Aqueous • Inflamed eyes, e.g., uveitis, have increased aqueous protein complements, and the aqueous may become plasmoid aqueous • Nonmalignant inflammatory conditions also show an increased albumin/globulin ratio • Ocular tumors can change the protein found in the aqueous: increased globulin and a decreased albumin/globulin ratio • High molecular weight proteins are sometimes found in the eyes of patients with glaucoma
Intraocular Pressure When Pressured, Keep Your Equilibrium!
Introduction • The outer wall of the human eyeball is partially elastic and encompasses fluids, the aqueous and vitreous humors • Given the optical purpose of the eye and the consequent need for precise and stable positioning of its refractive elements, regulation of the internal pressure is vitally important • The intraocular pressure (IOP) is kept within a narrow normal range by an equilibrium established between the production and drainage of aqueous • Small changes in the production or drainage of aqueous can create large IOP changes, for example, changes in the following may lead to IOP disturbance: force applied to the eyeball, body position, blood pressure, and central venous pressure
Aqueous Outflow • After its secretion into the posterior chamber by the ciliary epithelium, the aqueous passes between the back of the iris and the front of the lens, which may be touching, before passing through the pupil into the anterior chamber • Most of the aqueous leaves the eye through the trabecular meshwork and then through Schlemm’s canal, then into the external collector channels and eventually into the episcleral venous plexus – various amounts of resistance are met by this flow in the posterior chamber, the anterior chamber, entering into Schlemm’s canal, within the canal itself, and passing though the venous plexus
Aqueous Outflow 2 • If the aqueous is produced at a constant rate, the IOP will rise until it exceeds the outflow resistance • When the outflow resistance exactly equals the rate of aqueous production, the IOP will level off and stabilize – however, any change in the rate of production or drainage will upset this equilibrium • Aqueous is produced by the ciliary epithelium as a result of active pumping processes • These pumps are not affected by IOP, but their activity can be reduced through the use of beta-adrenergic blockers or carbonic anhydrase inhibitors
Aqueous Outflow 3 • The first element of resistance the aqueous encounters is between the iris and the lens – in some eyes there is a slight pressure difference between the posterior and anterior chambers, so that the middle of the iris may bow forward (physiologic iris bombé) • The aqueous then makes its way to the anterior angle (drainage angle) where it passes through the uveal meshwork into the corneo-scleral trabecular meshwork • Next it must negotiate the juxtacanalicular tissue and the endothelium lining of Schlemm’s canal to enter the canal itself • The trabecular meshwork, including the juxtacanalicular tissue, is the principal site of resistance to aqueous outflow
Aqueous Outflow 4 • Once past the canal, the aqueous passes through the external collector channels (except for the small amount that finds its way through the aqueous veins) into the deep scleral plexus, then into the intrascleral plexus and, finally, into the episcleral plexus • The combined resistance these venous structure present is equal to the episcleral venous pressure • The flow of the aqueous out the conventional route outlined above is pressure dependent and hydrodynamic, dependent on the hydrostatic pressure head and the resistance to outflow • (F = P C), where F is aqueous flow, P is the pressure difference, and C is the facility of aqueous outflow • The second path the aqueous can take out of the eye is the uveoscleral outflow – some aqueous, 10% to 20%, seeps through the face of the ciliary body in the angle recess of the anterior angle
Aqueous Outflow 5 • This uveoscleral outflow aqueous passes between the muscle fiber bundles and into the supraciliary space and eventually passes through the sclera or, via the suprachoroidal space, travels to the vortex veins • It might be expected that this uveoscleral flow would increase with increased pressure, but it is constant and independent of IOP – this may be due to the elevated IOPs compressing the uveal tissue against the sclera, preventing the higher pressure from increasing the outflow
IOP Measurement • Tonometers are the clinical instruments used to measure the IOP. • There are two types: 1) applanation, and 2) indentation • In applanation tonometry the force required to flatten a particular area of the cornea is determined • In indentation tonometry the amount of indentation caused by a probe carrying a known weight is determined • Applanation tonometry is most accurate and provides a direct measure of IOP since pressure is force per unit area and in applanation tonometry the force required to flatten a given area is precisely what is measured
Applanation Tonometry There are four sources of applanation error: • When a small area of the cornea is flattened, a small volume of aqueous is displaced – this makes the IOP seem larger than it actually is • The tear film forms a meniscus in the angle between the applanating surface and the cornea, and the area of the flattened cornea could be overestimated – this makes the IOP seem lower than it actually is • The surface tension of the tears adds a small amount of force to that of the tonometer – this makes the IOP seem lower than it actually is • A certain amount of force is required to flatten the cornea itself and this increases the force necessary to applanate a certain area of the cornea – this makes the IOP seem larger than it actually is
Goldmann Tonometer • Goldmann tonometry is the most accurate form of tonometry and is the clinical standard for IOP measurement • This tonometer was designed to minimize the four errors • The area of flattening is small so that the amount of aqueous displaced is minimal and only a minimal amount of the cornea is flattened • The area of applanation is only 3.06 mm and was selected because at this dimension the surface tension of the tear fluid and the mechanical resistance of the cornea cancel out (#3 cancels #4 on previous list) • Clinically, the tear meniscus is stained with fluorescein dye so that it will not be confused with the area of the cornea flattened • The applanating force necessary in grams times 100 gives the IOP in mm Hg
Goldmann Tonometry 2 • The flattened region of the cornea is viewed through a slit lamp, and the force against the cornea is increased until the inner border of the two halves of the double images just touch • Why is the image doubled? Why not just measure the size of the flattened region? • If direct measurement were used, eye movements, both voluntary (such as fixational) and involuntary (such as micronystagmus, drift, and microsaccades) would interfere – the image would constantly move and jiggle, making measurement impossible • By using prismatic doubling that amounts to 3.06 mm, both of the doubled images move in synchrony and it is an easy matter to align them—so when the area of flattening is 3.06 mm the doubled images will just touch
Goldmann Tonometry 3 • When the images are aligned, the flattened area exactly equals the prismatic doubling, the sought after 3.06 mm • The amount of prismatic doubling is equal to the distance from the center of one image to the center of the other image – a distance exactly equal to the size of the applanated area • This same principle, adopted for the same reason, to eliminate the effects of eye movements, is used in keratometers to measure anterior corneal curvature using an image formed by reflection from the front surface of the cornea
Indentation Tonometry • Indentationtonometry depends upon measuring the indentation of the cornea made by a polished probe that slides within a metallic footplate and carries a known weight • The Schiøtz tonometer is the best known indentation tonometer • Typically, anesthetic is applied to the cornea and the tonometer is allowed to rest on the cornea – the weighted plunger indents the cornea below the level of the footplate and the amount of indentation is mechanically indicated on a scale
Indentation Tonometry 2 • A major error is introduced by this form of tonometry, because the indentation significantly reduces the anterior chamber volume and this causes a large increase in the IOP, as much as 10 mm Hg – another error is due to the fact that the resistance of the cornea, the ocular rigidity, is more severe when the cornea is indented as compared to being applanated • Calibration charts have to be used that take this artificial (induced) IOP elevation into account in order to determine the actual IOP • Schiøtz tonometry is accurate, but more difficult to perform and is used only when Goldmann tonometry, or some other form of applanation tonometry, cannot be used
Tonography • Tonography is a procedure in which the Schiøtz tonometer is placed on the cornea and left there for four minutes • The weight increases the IOP, which increases the hydrostatic pressure head, pushing aqueous from the eye at a rate that is determined by the facility (of outflow) of the trabecular meshwork; consequently, the IOP gradually decreases with time • The initial scale reading and the final scale reading (taken after four minutes) are recorded, and the slope of the recording is used to determine the aqueous outflow facility • Tonography is not commonly used in the clinic, but has led to a better understanding of IOP in the various forms of glaucoma