Download
1 / 45
450 likes | 578 Views
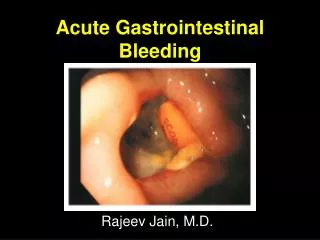
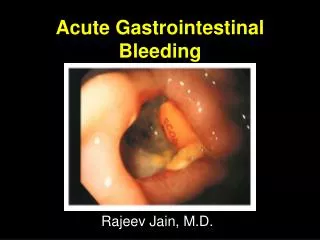
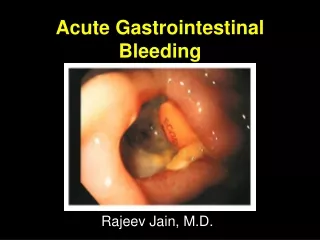
Hemetamesis and Hemetochezia (Acute GI Hemorrhage). Dr. Wu ShuMing GI Dept. RenJi Hospital SSMU. Five Ways of GI Bleeding. Hematemesis : vomitting of blood of altered blood ( coffee grounds ) indicates bleeding proximal to ligament of Treitz

E N D
Hemetamesis and Hemetochezia(Acute GI Hemorrhage) Dr. Wu ShuMing GI Dept. RenJi Hospital SSMU
Five Ways of GI Bleeding • Hematemesis:vomitting of blood of altered blood(coffee grounds) indicates bleeding proximal to ligament of Treitz • Melena:Tarry stool. Altered (black) blood per rectum (>60ml) • Hematochezia: Bright red or maroon rectal bleeding implies bleeding beyond Lig.T.* • FOB+ and Iron deficiency anemia
Factors affect the way to manifest • Site of bleeding • Speed of bleeding • Amount of blood loss • Flora of enterocolon .
Differentiating Upper from Low GI Bleeding • Hematochezia usually represents a lower GI source bleeding • Upper GI lesion may bleed so briskly that blood doesn`t remain in bowl long enough to become melena • Bleeding lesion distal to T Lig.may be either M.or hematochezia, but never manifests hematemesis
Common cause of up GI bleeding Peptic ulcer ; Gastropathy (alcohol, aspirin, NSAIDs, stress); GE varices; Gastric cancer
Less common cause of up GI bleeding Esophageal or intestinal neoplam Esophagitis; Malloy-weiss tear, Hemoptysis: Swallowed blood Anticoagulant fibrinoloytic therapy: Telangiectases; aneurysm ;vasculitis;Dieulafoy ulcer; AV malformation Connective tissue disease; Hemabilia(biliary origin;Crohn`s disease;amyloidosis , hematological diseases
BENIGN GASTRIC ULCER The classical presentation of gastric ulcer : with weight loss and indigestion made worse by eating, patients more often describe symptoms that would fit equally well for duodenal ulcer - investigation with barium meal or (preferably) endoscopy is, of course, appropriate for either. Benign ulcers may occur at any site in the stomach, but are commonest on the lesser curve away from acid-secreting epithelium.
Location of benign gastric ulcersin relationship to the distance from the pylorus. The majority of benign ulcers will be found on the lesser curvature within 3 cm of the angulus.
Duodenum Ulcer • The lesion most commonly affecting the duodenum is ulceration, and it is now known that both antral infection with Helicobacter pylori and the presence of gastric acid are virtual prerequisites for it..
Bleeding From EV • A number of cutaneous features (stigmata) may develop in a patient with cirrhosis, and these are important as they aid clinical recognition of chronic liver disease.
Bleeding Survey: Endoscopic Findings in 214 Patients With Clear Nasogastric Aspirates FINDING NUMBER OF PATIENTS INCIDENCE (%) Duodenaal ulcer 64 29.8 Gastric erosions 57 6.5 Gastric ulcer 47 21.9 Esophagitis 23 10.7 Duodenitis 21 9.8 Varices 11 5.1 Mallory-Weiss tear 10 4.7 Neoplasm 8 3.7 Stomal ulcer 7 3.3 Esophageal ulcer 2 0.9 Telangiectasia 0 Other 18 8.4
Clinical manifestation of GI Bleeding • Abdominal disconfort Nausea, • Hemadynamic change: reduction in blood volume (syncope,light-headedness, sweating,therst) or shock • Laboratory changes: HCT, BUN
Hematemesis with other symptoms • Hematemesis with upper abdominal pain • Hematemesis with hepatomegly and spleenomegly • Hematemesis with jaundice • Hematemesis with Skin & mucosa hemorrhage • Hematemesis with upper abdominal mass • Others: NSAIDs, Stress, Burning, Brain operation, Trauma, Vomiting
Lab.Examination in Localization & Diagnosis of GI Bleeding • Endoscopy • Barium Radiographs • Angiography • Radionuclide imaging
Approach to the patient with acute upper gastrintesttinal hemorrhage Acute upper Gastrointestinal Hemorrhage Rapid assessment Monitor hemodynamic status Fluid resuscitation Gastric lavage(?) self-limited (80%) bleeding (10-20%) Empiric medical therapy Urgent endoscopy recurrent hemorrhage endoscopy Site not localized Localized further assessment enteroscopy, radioisotope s scan, angiography, exploratory surgery Definitive therapyDefinitive therapy
Endoscopic view of a Mallory-Weiss tear with active bleeding (gastric lumen is at top left). B, Endoscopic view of an organized clot adherent to a Mallory-Weiss tear (gastric lumen is at bottom left ).
Endoscopic view of a Dieulafoy lesion on the lesser curvature of the stomach
Endoscopic view of a vascular ectasia (angiodysplasia) in the duodenum.
Endoscopic view of the gastric antrum with watermelon stomach. The pylorus is at top center. Note the linear distribution pattern of the vascular lesions arranged radially around the pylorus.
Endoscopic views of ulcers with stigmata of recent hemorrhage. A, Duodenal ulcer with a visible vessel. B, Gastric ulcer with a red spot in the center of the crater. C, Duodenal ulcer with a red spot in the center of the crater. D, Purplish clot adherent to a gastric ulcer.
Typical picture of a trivial nonsteroidal anti-inflammatory drug (NSAID)-induced injury to the gastric mucosa. There are multiple small erosions with brown-black staining of the center as a result of local bleeding and petechiae.
Typical round gastric ulcer at the angulus (incisura) of the stomach.
Differentiating Upper from Low GI Bleeding • Hematochezia usually represents a lower GI source bleeding • Upper GI lesion may bleed so briskly that blood doesn`t remain in bowl long enough to become melena • Bleeding lesion distal to T. Lig. may be either M.or hematochezia, but never manifests hematemesis
Hematochezia with other symptoms • Abdominal pain • Fever • Tenesmus • Systemic Hemorrhage • Dermal sign • Abdominal mass
Lab. Examination For detecting Low GI Bleeeding • Anoscopy & sigmoidoscopy • Barium Edema (BE) • Angiography • Radionuclide scanning
A, Linear ulcers of Crohn's colitis. B, Mucosa surrounding the ulcers is nodular (cobblestoning).
Shigella colitis. Patchy areas of erythema, spontaneous bleeding, and loss of the normal vascular pattern are evident
Salmonella colitis. Diffuse erythema, spontaneous bleeding, and loss of the vascular pattern with formation of telangiectasis are present.
Tuberculosis. Linear ulceration runs circumferentially along the interhaustral septum with tiny satellite ulcerations. This must be distinguished from the longitudinal linear ulcerations seen in inflammatory bowel disease.
Pseudomembranous (antibiotic-associated) colitis. Numerous elevated yellowish plaques are present on the mucosal surface.
Amebiasis. Discrete punched-out ulcers are present in the right colon.
Severe acute ulcerative colitis. No vascular pattern is discernible. A severe degree of spontaneous bleeding is present
Barium enema appearance of an ischemic stricture with features of carcinoma: asymmetry, mucosal destruction, and shouldering.
Summary of Acute GI Bleeding • Upper GI source bleeding--Hemetemesis • Major upper GI bleding-- Hemetemesis & hemetochezia • The more distant from the rectum, the more likely that melaena occurs • The colon lesion--FOB+ or hemetochezia • The small bowl lesion-- melena or hemetochezia
The questions should be posed • Prior bleeding episode? • Family history of GI diseases • Dose the patient have the illness of ulcer? Cirrhosis?cancer?bleeding disorder? • Alcohol? NSAIDs? • Any precedes symptoms or signs?