Download
1 / 2
20 likes | 205 Views
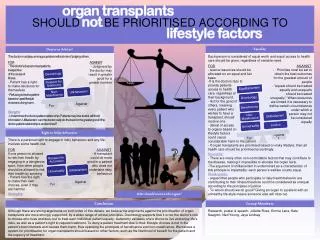
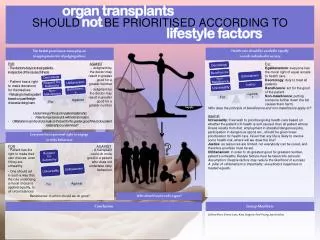
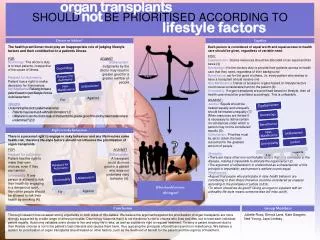
organ transplants. SHOULD not BE PRIORITISED ACCORDING TO. lifestyle factors. Doctor or Arbiter?. Equal Access. Each person should be considered of equal worth and given equal access to health care, regardless of variable need. FOR:

E N D
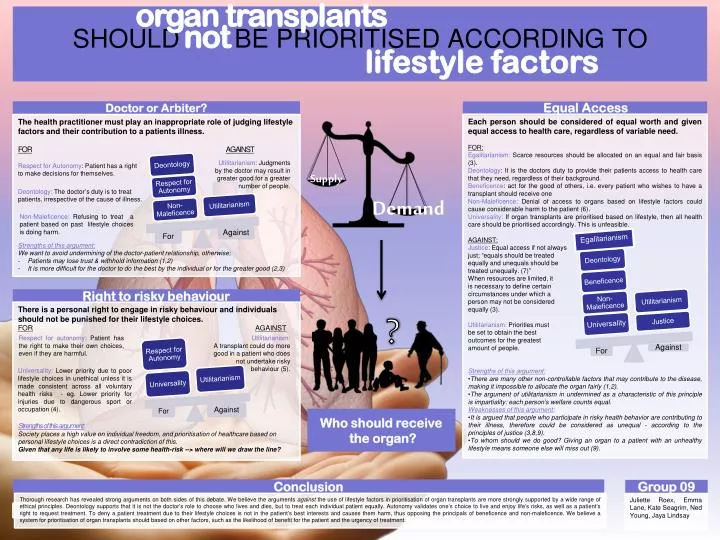
organ transplants SHOULDnotBE PRIORITISED ACCORDING TO lifestyle factors Doctor or Arbiter? Equal Access • Each person should be considered of equal worth and given equal access to health care, regardless of variable need. • FOR: • Egalitarianism: Scarce resources should be allocated on an equal and fair basis (3). • Deontology: It is the doctors duty to provide their patients access to health care that they need, regardless of their background. • Beneficence: act for the good of others, i.e. every patient who wishes to have a transplant should receive one • Non-Maleficence: Denial of access to organs based on lifestyle factors could cause considerable harm to the patient (6). • Universality: If organ transplants are prioritised based on lifestyle, then all health care should be prioritised accordingly. This is unfeasible. • AGAINST: • Justice: Equal access if not always • just; “equals should be treated • equally and unequals should be • treated unequally. (7)” • When resources are limited, it • is necessary to define certain • circumstances under which a • person may not be considered • equally (3). • Utilitarianism: Priorities must • be set to obtain the best • outcomes for the greatest • amount of people. • Strengths of this argument: • There are many other non-controllable factors that may contribute to the disease, making it impossible to allocate the organ fairly (1,2). • The argument of utilitarianism in undermined as a characteristic of this principle is impartiality: each person’s welfare counts equal. • Weaknesses of this argument: • It is argued that people who participate in risky health behavior are contributing to their illness, therefore could be considered as unequal - according to the principles of justice (3,8,9). • To whom should we do good? Giving an organ to a patient with an unhealthy lifestyle means someone else will miss out (9). • The health practitioner must play an inappropriate role of judging lifestyle factors and their contribution to a patients illness. • FORAGAINST • Strengths of this argument: • We want to avoid undermining of the doctor-patient relationship, otherwise; • Patients may lose trust & withhold information (1,2) • It is more difficult for the doctor to do the best by the individual or for the greater good (2,3) Utilitarianism: Judgments by the doctor may result in greater good for a greater number of people. Respect for Autonomy: Patient has a right to make decisions for themselves. Deontology: The doctor’s duty is to treat patients, irrespective of the cause of illness. Egalitarianism Supply Non-Maleficence: Refusing to treat a patient based on past lifestyle choices is doing harm. Demand Right to risky behaviour There is a personal right to engage in risky behaviour and individuals should not be punished for their lifestyle choices. FORAGAINST ? Respect for autonomy: Patient has the right to make their own choices, even if they are harmful. Utilitarianism: A transplant could do more good in a patient who does not undertake risky behaviour (5). Universality: Lower priority due to poor lifestyle choices in unethical unless it is made consistent across all voluntary health risks - eg. Lower priority for injuries due to dangerous sport or occupation (4). Who should receive the organ? Strengths of this argument: Society places a high value on individual freedom, and prioritisation of healthcare based on personal lifestyle choices is a direct contradiction of this. Given that any life is likely to involve some health-risk --> where will we draw the line? Conclusion Group 09 Thorough research has revealed strong arguments on both sides of this debate. We believe the arguments against the use of lifestyle factors in prioritisation of organ transplants are more strongly supported by a wide range of ethical principles. Deontology supports that it is not the doctor’s role to choose who lives and dies, but to treat each individual patient equally. Autonomy validates one’s choice to live and enjoy life’s risks, as well as a patient’s right to request treatment. To deny a patient treatment due to their lifestyle choices is not in the patient’s best interests and causes them harm, thus opposing the principals of beneficence and non-maleficence. We believe a system for prioritisation of organ transplants should based on other factors, such as the likelihood of benefit for the patient and the urgency of treatment. Juliette Roex, Emma Lane, Kate Seagrim, Ned Young, Jaya Lindsay
References 1.Sharkey KS, Gillam L. Should patients with self inflicted illness receive lower priority in access to health care resources? Mapping out the debate. Journal of Medical Ethics vol. 36 (2010): 661-665 2.Ho D, When Good Organs Go To Bad People. Bioethics vol.22 no.2 (2008): 77-83 3.Beauchamp TL, Childress JF. Principles of Biomedical Ethics, Oxford University Press (2001) 5th edn. 4.Brudney D. Are Alcoholics Less Deserving of Liver Transplants? Hasting Centre Report vol. 37 no.1 (2007): 41-47 5.McMaster P. Transplantation for alcoholic liver disease in an era of organ shortage. The Lancet vol.335 (2000): 424-425 6.Council on Ethical and Judicial Affairs, American Medical Association. Ethical Considerations in the Allocation of Organs and Other Scarce Medical Resources Among Patients. Archive of Internal Medicine vol.155 (1995): 29-40 7.Rogers WA, Braunack-Mayer. Practical ethics for General Practice, Oxford University Press (2009) 2nd edn. 8. Kluge E. Drawing the ethical line between organ transplantation and lifestyle abuse. Canadian Medical Association Journal vol.150 no.5 (1994): 745-6 9. Thornton V. Who gets the liver transplant? The use of responsibility as a tie breaker. Journal of Medical Ethics vol. 35 (2009)