Download
1 / 47
490 likes | 844 Views
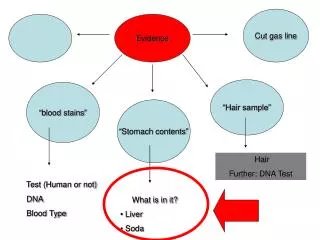
Evidence. Good vs. bad. Systematic reviews & Meta-analyses. Randomized controlled double blind studies. Evidence Pyramid a "hierarchy of evidence". Cohort studies. As you move up the pyramid the amount of available literature decreases, but increases in relevance to the

E N D
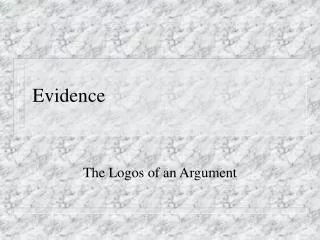
Evidence Good vs. bad
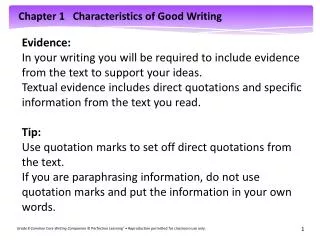
Systematic reviews & Meta-analyses Randomized controlled double blind studies Evidence Pyramida "hierarchy of evidence" Cohort studies As you move up the pyramid the amount of available literature decreases, but increases in relevance to the clinical setting Case-control studies Case series Case reports Ideas, editorials, opinions Animal research
Using the Evidence Pyramid • Start from the top and work down to find the highest quality evidence available • Systematic reviews and meta-analyses provide the most useful information • If that type of information isn’t available, move down the pyramid to cohort, case-control, case series, etc.
Systematic review • A comprehensive survey of a topic in which all of the primary studies of the highest level of evidence have been systematically identified, appraised and then summarized according to an explicit and reproducible methodology
Meta-analysis • A survey in which the results of all of the included studies are similar enough statistically that the results are combined and analyzed as if it was one study • A good systematic review or meta-analysis will be a better guide to practice than an individual article (usually)
Meta-analysis Statistically
Meta-analysis pitfalls • Rare for the results of different studies to agree precisely • If authors want to support a particular conclusion, they can include studies that support that conclusion and omit studies that don’t • Studies that show a positive effect tend to be published more often than those that do not • If authors include only published studies, several weak positive studies may seem to add up to a strong positive result
Randomized controlled study • Involves a treatment group and a control group • Treatment group receives the treatment • Control group receives either no treatment or a standard treatment • Patients are randomly assigned to groups • Assigning patients at random • Reduces the risk of bias • Increases the probability that differences between the groups can be attributed to the treatment
RCT pitfalls • Often the methods utilized in RCTs are different from what is commonly practiced in the clinic • Patients are often different than those commonly seen by practitioners • The setting is often different
Cohort Study • A study in which patients who presently have a certain condition and/or receive a particular treatment are followed over time and compared with another group who are not affected by the condition/treatment
Cohort Study Pitfalls • Cohort studies are not as reliable as randomized controlled studies • They can take a very long time to complete, since the researchers have to wait for the conditions of interest to develop • Other things tend to change over the course of the study tending to confound the study’s results • People don’t live in a vacuum
Case control study • Patients who already have a certain condition are compared with people who do not
Case control study pitfalls • Less reliable than either RCTs or cohort studies • Just because there is a statistical relationship between conditions does not mean that one actually caused the other • Coffee drinking is related to lung cancer • Smoking is more common in coffee drinkers • Researchers will typically try to confirm results with a RCT or a cohort study
Chiropractic Manipulation and Stroke A Population-Based Case-Control Study Rothwell et al. Stroke. 2001;32:1054-1060.
Case series and case reports • Collections of reports on the treatment of individual patients, or of reports on a single patient • May provide information that will assist in a diagnosis or to see how others have managed a certain condition
Case series and reports pitfalls • Have no statistical validity because they use no control group with which to compare the results of the study • Better evidence should be available for any reasonably well-known condition • They frequently identify new conditions leading to more rigorous methods of investigation
Current Evidence in Chiropractic • Use • Cost • e.g., Legorreta study • Safety • Efficacy • Very little evidence on which types of spinal manipulation (techniques) are most beneficial
Evidence-based Chiropractic • Same fundamental ideas & practices as other HC providers using EBP • Framed in the philosophy of chiropractic (a chiropractic paradigm) • Questions to ask are based on this paradigm • Impacts our view of the world of health care • Required to make common sense of research & scholarship (evidence)
EBC cont. • Uses philosophy to interpret research & scholarship • But EBC itself is not a philosophy of chiropractic • It is a manner of practicing healthcare
EBC cont. • Making health care decisions is an ongoing practice • Because knowledge gained in school ages and becomes obsolete • Science changes
Does that mean that philosophy and evidence are incompatible?
NO! • We ground our practice in our philosophy and belief system • Dictionary definition of evidence: • Grounds for belief • Knowledge on which to base belief • So: Evidence can provide a basis in fact for our beliefs
Publishing in chiropractic = “Getting the word out!” • DD Palmer • “The Chiropractor” • Still holds the record for the longest-lived chiropractic periodical (57 years) • Solon Massey Langworthy • Founder-American School of Chiropractic • Co-published first textbook of chiropractic, Modernized Chiropractic (1906)1 1. Smith OG, Langworthy SM, Paxson M. Modernized chiropractic. Cedar Rapids, IA: Laurance Press, 1906.
Publishing in chiropractic cont. • BJ Palmer • Books, pamphlets & periodicals published via his own print shop • Over 70 books, hundreds of pamphlets, several periodicals • Also a commercial radio venture (WOC)
Chiropractic reading material • Popular press (DC) • National associations have published journals for decades • Mostly not peer-reviewed • JACA has peer-reviewed Research & Science section • Journals of Canadian and Australian Associations
Chiropractic reading material cont. • Newsletters, magazines & journals from state associations, colleges, non-profits, technique groups, practice-management consultants, etc. • Indexed, peer-reviewed journals • Chiropractic, medical, PT, osteopathy, CAM • Represents a higher level of evidence
Original research,AKA pure research • Produces new knowledge • Adds something new & unique to the storehouse of human knowledge • AKA “the evidence base” • Usually done by highly educated and/or experienced people in practice, government, & universities • Conducted by empirical or oral methods
Oral vs. Empirical research methods • Empirical research • Is based on observed and measured phenomena • Derives knowledge from actual experience rather than from theory or belief • Oral method of original research • Directly communicating with people • Interviews, surveys, polls, questionnaires • Recording perceptions, opinions, beliefs
Bibliographic research • Analyze what others have written • Gather information from published materials • Reach your own interpretation of conclusions • Literature reviews • Educational articles
EBC – better with experience • EBC starts with asking patient-oriented, clinically relevant questions • Expert clinicians generate better questions than novice physicians (Norman 1988) • Experts have more experiences from which to draw upon to formulate questions
Experience cont. • Clinical experience is valuable in the critical appraisal process • Experience can be drawn upon to determine if the literature is applicable to the current clinical context • EBC = clinical experience + best available evidence + patient values
Better with experience? • There is a statistically and clinically significant negative correlation between knowledge of up to date care and the years elapsed since graduation from medical school (Hasn’t been studied for DCs, but . . . )
Practice guidelines: Friend or Foe? Are they just picking on us?
Clinical Practice Guidelines • Systematically developed statement designed to assist practitioners and patients make decisions about appropriate health care for specific clinical circumstances • Often used to approve care • By insurance companies • Regulating bodies
Evidence: who cares about it? • Patients/consumers • Payors (insurance/case managers) • Other providers • Government • Academic institutions • Allied health professions
Patients want evidence • It is increasingly common for patients to expect you to address information they have obtained from friends etc. • Not just about chiropractic, but about any issues that affect their health • They use the Internet, books, magazines, journals • They need the chiropractor’s help in interpreting and evaluating it
What do you mean “It works”? • Patient • Convenient, effective, satisfying • Clinician • Efficient, effective, safe, satisfying • Clinical Scientist • Quantify effect size, efficacy compared to placebo or no treatment, safety
Two common pitfalls • The artificial authority of quotation marks • Opposite mistake: • If information about a procedure is not in the literature, then that practice cannot be used • Lack of evidence does not mean evidence of lack • Logical reasoning is required of the practitioner
All providers will be expected to provide evidence • FDA has required drug trials for many years • Surgical procedures are being criticized for lack of evidence • Chiropractic has more evidence than many medical or surgical procedures • Example: AHCPR back pain guidelines
EBC and referrals from medical practitioners • In order to recommend treatment • Harmfulness (disutility) of the treatment must be lower than the disutility of the illness • High probability that the treatment will be successful • If a condition is worse than the risks, costs, and nuisance of a treatment, then that treatment is warranted
Medical referrals cont. • Chiropractic is relatively safe, inexpensive, and noninvasive, and therefore has a low level of disutility • Some neurologists are distorting the evidence concerning the potential for manipulation to cause disc herniations and stroke