Download
1 / 58
670 likes | 1.3k Views
PORTAL HYPERTENSION. PRESENTER: KRITHIKA KRISHNAN MODERATOR : DR.R.PANDEY. www.anaesthesia.co.in anaesthesia.co.in@gmail.com. Mr. Anil Kumar Rai; 36yrs / male; Vendor; New Delhi; Presenting complaints. Vomiting of blood Black tarry stools 1 month back

E N D
PORTAL HYPERTENSION PRESENTER: KRITHIKA KRISHNAN MODERATOR : DR.R.PANDEY www.anaesthesia.co.inanaesthesia.co.in@gmail.com
Mr. Anil Kumar Rai; • 36yrs / male; • Vendor; • New Delhi; • Presenting complaints • Vomiting of blood • Black tarry stools 1 month back • Loss of consciousness
History of presenting complaints • Vomiting of blood. • 2 episodes. • 50 ml each. • Dark colour mixed with fresh blood. • Not associated with cough. • Passage of black tarry stools. • 2 episodes.
H/O Loss of consciousness. • 1 episode. • Not associated with trauma. • Lasted for 30 seconds. • H/O abdominal distension. • 1 month. • Progressively increasing. • Uniform. • Not associated with abdominal pain.
H/O yellowish discolouration of the body and mucous membrane • 1 month. • Progressively deepening. • Not associated with clay stools or dark urine. • H/O fever… 1 month • Low grade. • Intermittent. • Relieved with drugs.
H/O wakefulness in night and day time sleepiness. • 15 days back. • Improved with medications. • H/O loss of weight. • 15 kgs over past 2 years. • H/O loss of appetite.
No H/O…. • Pedal edema. • Breathlessness on exertion. • Chest pain. • Palpitation. • Decreased urine output. • Bruising/ gum bleed .
Personal History • Consumes mixed diet. • Chronic alcoholic since 15 years of age, stopped one year back (8-10 pegs of country liquor/day). • H/O smoking since 15 years of age, stopped one year back – about 15 pack- years. • No H/O drug abuse.
Treatment History • H/O upper GI endoscopy and sclerotherapy. • Repeated paracentesis for the ascites. • Antibiotics. • T. Aldactone 100mg OD. • T. Methyl cobalamine1500mg OD. • T. Thiamine 100mg OD. • Syrup. Lactulose 30ml TDS.
Past History • H/O similar episodes of hemetemesis present …2 years • 4 such episodes. • UGI endoscopy done….diagnosed as oesophageal varices and sclerotherapy done. • Evaluated and diagnosed as cirrhosis with ESLD. • H/O spontaneous bacterial peritonitis. • 6 months back. • Treated with antibiotics.
No H/O any other systemic illness. • No H/O any surgery in the past. Family History • No H/O any similar illness in the family.
55 kg, 5 feet 7 inches. Average built . Pallor +ve. Icteric. No clubbing. No cyanosis. No pedal edema. No other sign of liver cell failure. No significant lymphadenopathy. Venous access - good General examination
Vital Signs • Pulse rate • 72 beats/ min, • regular in rhythm, • normal in volume and character. • Blood pressure • 120/60 mm Hg • measured in right upper limb ,in the supine posture. • Jugular venous pulsations visible, pressure not elevated. • Temperature - 37ºC.
AirwayExamination • MMP II. • Mouth opening and neck movements adequate. • No loose tooth/ artificial denture. • TMD >3 fingers.
Systemic examination Abdomen On inspection • Distended uniformly. • All quadrants moving equally with respiration. • No dilated veins. • Needle prick scars made out in the flanks. • Umbilicus – inverted. • Divarication of recti present.
On palpation • Soft. • No tenderness. • Spleen palpable below the left costal margin up to the umbilicus. • Liver – not palpable. On percussion • Shifting dullness present. • Liver span – 7 cm.
Cardiovascular System • S1 S2 heard - normal, no murmurs. Respiratory System • B/L vesicular breath sounds present, no added sounds. Central Nervous System • Clinically normal.
Provisional diagnosis Decompensated chronic liver disease with portal hypertension with ascites.
Investigation: Hemogram Hb :9 g/dl TLC 3700/cumm DLC P 74, L 23, M 2 Platelet 71000/cumm PT 12/16.2
Biochemistry Blood sugar (R): 152 mg/dl B.Urea: 103 mg/dl S. Creatinine: 1.9 mg/dl Na+/K+: 141/4.1 meq/L S.Bilirubin: 3 mg/dl 0.8mg/dl 2.2mg/dl SGOT/PT 76/56 ALKPO4 222 T.Proteins/ Albumin/globulin: 7.7/4.0/3.7 Unconjugated Conjugated
CXR : WNL • ECG : WNL • Echo : Normal study • USG abdomen: Liver small in size with slightly coarse echotexture. • UGI endoscopy: Grade III esophageal varices. • CECT : atrophy of R lobe of liver , spleen enlarged with infarct. • HBsAg -ve. • Anti HCV antibodies –ve.
Final diagnosis Decompensated chronic liver disease, probably alcohol in etiology, with portal hypertension with ascites.
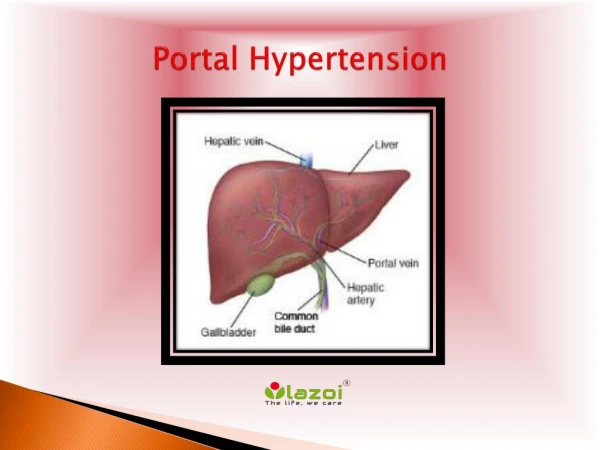
Portal hypertension(>10mmHg) and its consequences • Gastroesophageal varices • Ascites • Hepatic encephalopathy • SBP • Hepatorenal syndrome • HCC
Laboratory findings (minimal or absent) • Anemia (a frequent finding) • Coagulation abnormalities • Increased AST, ALP, bilirubin, gamma globulins • Decreased albumin
Imaging: • Spleen and hepatic enlargment • Barium / endoscopic studies- presence of varices • USG/ CT/ MRI –for liver size, ascitis, hepatic nodules • Doppler- for assessing the patency of splenic, portal & hepatic veins
Portal Hypertension: • Hemorrhage from varices. • Splenomegaly with hypersplenism. • Ascites. • Acute and chronic hepatic encephalopathy.
Diagnosis: • Fibreoptic esophagoscopy -for confirming varices. • MRI and contrast CT- tool for detecting the collateral circulation. • Percutaneous transhepatic catheterisation-Portal venous pressure.
Management of acute bleed • Prompt replacement of fluid loss • Replacement of clotting factors with fresh frozen plasma • Monitoring of CVP or cap.wedge pressure • Vasoconstrictors • Balloon tamponade • Endosopic variceal ligation • Sclerotherapy • Gastric devascularisation
Pathological feaures in advanced liver disease: 1.Hyperdynamic circulation ↓ peripheral vascular resistance ↑ cardiac output Other CVS changes Increased SV & HR. Normal filling pressures. Decreased sensitivity to vasopressors. Cardiomyopathy.
2. Hypoxemia: • Intrapulmonary shunting • Precapillary sphincter dilatation (HPS I). • AV shunting (HPS II). • V-Q abnormality in the lung. • Exacerbated in the upright position. • Pleural effusion. • Pulmonary infection. • Diaphragmatic dysfunction. • Dysfunction of HPV. • Rightward shift of O2 dissociation curve.
3. Metabolic alkalosis: High aldosterone state. 4. Coagulation abnormalities: Deficiency of plasma clotting factors. ↓ platelet count. ↓ platelet function. Abnormal fibrinolytic factors.
5. Hepatic blood flow • Summation of hepatic arterial & portal venous blood flow • Effect of anesthetic drugs • Ventilation – IPPV, CO2 • Effect of surgery 6. Ascites 7. Renal impairment 8. Hepatic encephalopathy
Underfill hypothesis Overflow hypothesis Treatment Spirnolactone Paracentesis, large volume ± albumin Frusemide Peritoneovenous shunt Ascites
HPS Presence of chronic disease Absence of intrinsic cardiopulmonary disease Pulmonary gas exchange abnormality Intrapulmonary vascular dilatation PPH PAP >25mmHg PCWP <15mmHg PVR >120 dynes/s/cm5 Hepatopulmonary syndrome
Hepatorenal syndrome International ascites club criteria 1. S.creatinine >1.5mg/dl (133 µmol/l), GFR <40ml/min. 2. Absence of on going bact infection, fluid loss, treatment with nephrotoxic drugs. 3. No sustained improvement after diuretic withdrawal and plasma volume expansion. 4. Proteinuria < 0.5g/dl. 5. No USG evidence of parenchymal renal disease. • U. Na+ <10 • U.sediments: N • U.osmolality: exceeds pl osmolality by atleast 100mosm/l • U/Pl cr. ratio >30:1
Hypoxia. Hypovolemia. Hypoglycemia. Anemia. Infection, pneumonia sepsis. UGI bleed. Increased protein intake. Constipation. Large volume parcentesis. Diarrhea and vomiting. Diuretic. Sedatives. Shunts. Treatment Avoid ppt factors. Lactulose. Neomycin . Metronidazole. Liver transplantation. Precipitating factor
Guidelines for anaesthetic management in patients with ESLD Common operative procedures: Surgery for gastric/duodenal ulcer, cholecystectomy, & colon carcinoma Various orthopedic procedures Portocaval shunts, Sclerotherapy, gastric devascularisation surgery
Preoperative instructions – • NPO > 8 hours. • High risk consent in the view of perioperative risk of renal and hepatic failure. • Hydration of the patient with IV fluids @100ml/hour. • CM S.electrolytes, PT and platelets. • Premedication with T.Lorazepam 4mg HS & CM and T.Ranitidine 150mg HS & CM.
Induction: Mod RSI • Pre oxygenation for 3 minutes. • Titrated dose of propofol (Thio can also be used). • Intubate after giving scoline. • Maintenance :- • Volatile agents: Isoflurane, desflurane or sevoflurane. • NMB: Non depolarizing agents - Altered Vdss.
Opioids: Fentanyl. Morphine. Pain: Best controlled with epidural opioids if CNB is not contraindicated.
Risk assessment in patients with liver diseaseChild – Pugh score
MELD score: MELD = 3.8 x loge(bil ) + 11.2 x loge(INR) + 9.6 x loge(creatinine) Causes of mortality in the periop period: Sepsis, pneumonia. Renal failure. Non mechanical bleeding. Hepatic failure & encephalopathy.
Liver transplantation • Indications • Children. • Adults. • Contraindications • Absolute. • Relative.
Preoperative preparation • Central nervous system status. • Encephalopathy grade. • ICP. • Coagulation status. • Renal failure. • Cardiopulmonary status.
Phases of OLT • Preanhepatic phase • Monitor placement to clamping. • Medications titrated. • Lorazepam, morphine, oxazepam. • Temperature monitoring and maintenance. • Invasive monitoring. • Defibrillator ready. • Rapid infusor. • Thromboelastography. • Periodic blood sampling.
Anhepatic phase • Occlusion of vascular supply to old liver to perfusion of new liver. • Metabolic acidosis/ alkalosis. • Hypocalcemia. • Hypokalemia.
Postanhepatic phase • After perfusion of the new liver. • Ventricular fibrillation - hyperkalemia. • Hypotension – vasoactive amines. • Air embolism. • Paradox – Hepatic congestion.