Download
1 / 1
10 likes | 139 Views
No. 024. A comparison of prostate tumour volume estimation methods: Which method is best in routine clinical practice?. Marlon Perera 1 , Damien Bolton 2 and David Clouston 3 1 Western General Hospital, Footscray , VIC

E N D
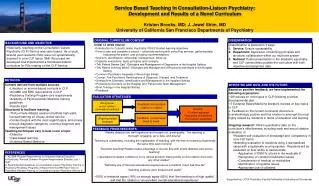
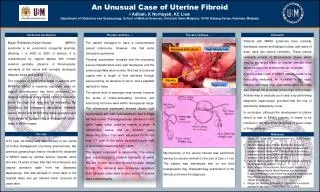
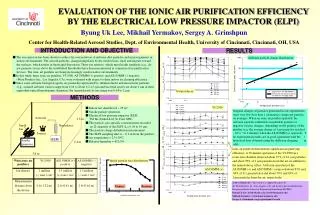
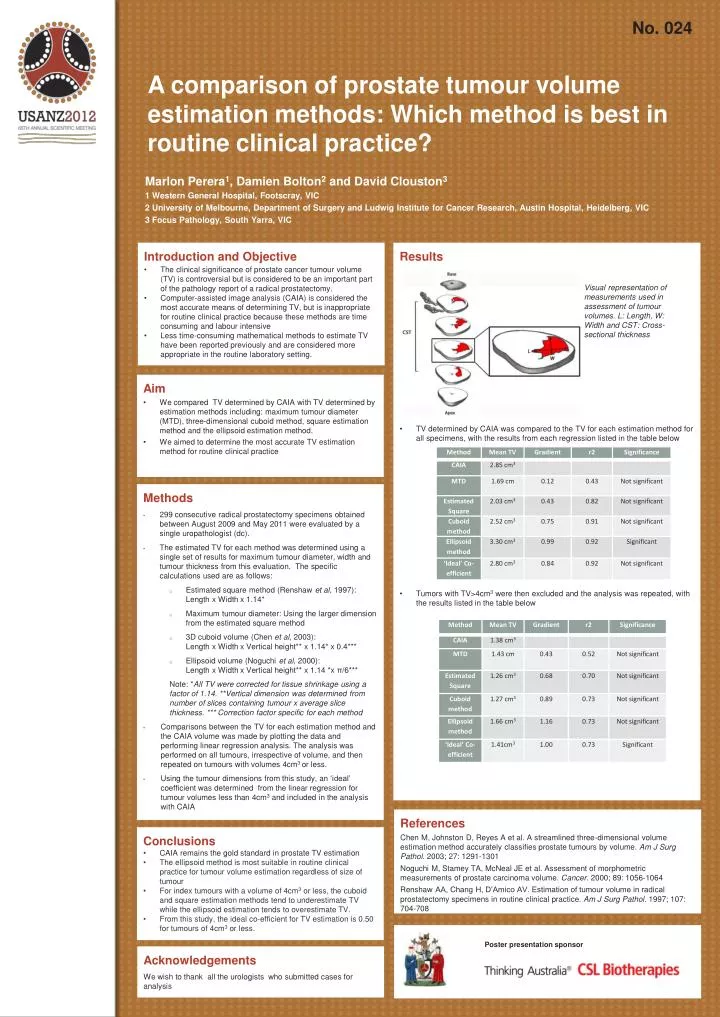
No. 024 A comparison of prostate tumour volume estimation methods: Which method is best in routine clinical practice? Marlon Perera1, Damien Bolton2 and David Clouston3 1 Western General Hospital, Footscray, VIC 2 University of Melbourne, Department of Surgery and Ludwig Institute for Cancer Research, Austin Hospital, Heidelberg, VIC 3 Focus Pathology, South Yarra, VIC • Introduction and Objective • The clinical significance of prostate cancer tumour volume (TV) is controversial but is considered to be an important part of the pathology report of a radical prostatectomy. • Computer-assisted image analysis (CAIA) is considered the most accurate means of determining TV, but is inappropriate for routine clinical practice because these methods are time consuming and labour intensive • Less time-consuming mathematical methods to estimate TV have been reported previously and are considered more appropriate in the routine laboratory setting. • Results • TV determined by CAIA was compared to the TV for each estimation method for all specimens, with the results from each regression listed in the table below • Tumors with TV>4cm3 were then excluded and the analysis was repeated, with the results listed in the table below Visual representation of measurements used in assessment of tumour volumes. L: Length, W: Width and CST: Cross-sectional thickness • Aim • We compared TV determined by CAIA with TV determined by estimation methods including: maximum tumour diameter (MTD), three-dimensional cuboid method, square estimation method and the ellipsoid estimation method. • We aimed to determine the most accurate TV estimation method for routine clinical practice • Methods • 299 consecutive radical prostatectomy specimens obtained between August 2009 and May 2011 were evaluated by a single uropathologist (dc). • The estimated TV for each method was determined using a single set of results for maximum tumour diameter, width and tumour thickness from this evaluation. The specific calculations used are as follows: • Estimated square method (Renshawet al, 1997): Length x Width x 1.14* • Maximum tumour diameter: Using the larger dimension from the estimated square method • 3D cuboid volume (Chen et al, 2003): Length x Width x Vertical height** x 1.14* x 0.4*** • Ellipsoid volume (Noguchi et al, 2000): Length x Width x Vertical height** x 1.14 *x π/6*** • Note: *All TV were corrected for tissue shrinkage using a factor of 1.14. **Vertical dimension was determined from number of slices containing tumour x average slice thickness. *** Correction factor specific for each method • Comparisons between the TV for each estimation method and the CAIA volume was made by plotting the data and performing linear regression analysis. The analysis was performed on all tumours, irrespective of volume, and then repeated on tumours with volumes 4cm3 or less. • Using the tumour dimensions from this study, an ‘ideal’ coefficient was determined from the linear regression for tumour volumes less than 4cm3 and included in the analysis with CAIA References Chen M, Johnston D, Reyes A et al. A streamlined three-dimensional volume estimation method accurately classifies prostate tumours by volume. Am J Surg Pathol. 2003; 27: 1291-1301 Noguchi M, Stamey TA, McNeal JE et al. Assessment of morphometric measurements of prostate carcinoma volume. Cancer. 2000; 89: 1056-1064 Renshaw AA, Chang H, D’Amico AV. Estimation of tumour volume in radical prostatectomy specimens in routine clinical practice. Am J Surg Pathol. 1997; 107: 704-708 • Conclusions • CAIA remains the gold standard in prostate TV estimation • The ellipsoid method is most suitable in routine clinical practice for tumour volume estimation regardless of size of tumour • For index tumours with a volume of 4cm3 or less, the cuboid and square estimation methods tend to underestimate TV while the ellipsoid estimation tends to overestimate TV. • From this study, the ideal co-efficient for TV estimation is 0.50 for tumours of 4cm3 or less. Poster presentation sponsor Acknowledgements We wish to thank all the urologists who submitted cases for analysis