Download
1 / 61
610 likes | 755 Views
Chapter 18 Lecture Outline. Functions of GI Tract. 18-5. Motility. Is movement of food through GI tract by means of: Ingestion --taking food into mouth Mastication --chewing food and mixing it with saliva Deglutition --swallowing food

E N D
Chapter 18 Lecture Outline
Motility • Is movement of food through GI tract by means of: • Ingestion--taking food into mouth • Mastication--chewing food and mixing it with saliva • Deglutition--swallowing food • Peristalsis--rhythmic wave-like contractions that move food through GI tract 18-6
Secretion • Includes release of exocrine and endocrine products into GI tract • Exocrine secretions include: HCl, H2O, HCO3-, bile, lipase, pepsin, amylase, trypsin, elastase, and histamine • Endocrine includes hormones secreted into stomach and small intestine to help regulate GI system • e.g. gastrin, secretin, CCK, GIP, GLP-1, guanylin, VIP, and somatostatin 18-7
Absorption Digestion Refers to breakdown of food molecules into smaller subunits • Is passage of digested end products into blood or lymph 18-8
Storage and Elimination • Includes temporary storage and subsequent elimination of indigestible components of food Immune Barrier Includes physical barrier formed by tight junctions between cells of small intestine And cells of the immune system that reside in connective tissue just below epithelium 18-9
Digestive System continued • Organs include oral cavity, pharynx, esophagus, stomach, and small and largeintestine • Accessory organs include teeth, tongue, salivary glands, liver, gallbladder, and pancreas 18-12
Layers of GI Tract 18-13
Mucosa • Is the absorptive and secretory layer lining lumen of GI tract • In places is highly folded with villi to increase absorptive area • Contains lymph nodules, mucus-secreting goblet cells, and thin layer of muscle 18-14
Submucosa • Is a thick, highly vascular layer of connective tissue where absorbed molecules enter blood and lymphatic vessels • Contains glands and nerve plexuses (submucosal plexus) that carry ANS activity to muscularis mucosae of small and large int. 18-15
Muscularis • Is responsible for segmental contractions and peristaltic movement through GI tract • Has an inner circular and outer longitudinal layer of smooth muscle • Activity of these layers moves food through tract while pulverizing and mixing it • Myenteric plexus between these layers is major nerve supply to GI tract • Includes fibers and ganglia from both Symp and Parasymp systems 18-16
Serosa • Is outermost layer; serves to bind and protect • Consists of areolar connective tissue covered with layer of simple squamous epithelium 18-17
From Mouth to Stomach 18-19
From Mouth to Stomach • Mastication (chewing) mixes food with saliva which contains salivary amylase • An enzyme that catalyzes partial digestion of starch 18-20
From Mouth to Stomach continued • Deglutition (swallowing) begins as voluntary activity • Oral phase is voluntary and forms a food bolus • Pharyngeal and esophagealphases are involuntary and cannot be stopped • To swallow, larynx is raised so that epiglottis covers entrance to respiratory tract • A swallowing center in medulla orchestrates complex pattern of contractions required for swallowing 18-21
From Mouth to Stomach continued • Peristalsis propels food thru GI tract • = wave-like muscular contractions • After food passes into stomach, the gastroesophageal sphincter constricts, preventing reflux 18-23
Stomach 18-24
Stomach • Is most distensible part of GI tract • Empties into the duodenum • Functions in: storage of food; initial digestion of proteins; killing bacteria with high acidity; moving soupy food mixture (chyme) into intestine 18-25
Stomach continued • Is enclosed by gastroesophageal sphincter on top and pyloric sphincter on bottom • Is divided into 3 regions: • Fundus • Body • Antrum 18-26
Stomach continued • Inner surface of stomach is highly folded into rugae • Contractions of stomach churn chyme, mixing it with gastric secretions • Eventually these will propel food into small intestine 18-27
Stomach continued • Gastric mucosa has gastric pits in its folds • Cells that line folds deeper in the mucosa, are exocrine gastric glands 18-28
Stomach continued • Gastric glands contain cells that secrete different products that form gastric juice • Goblet cells secrete mucus • Parietal cells secrete HCl and intrinsic factor (necessary for B12 absorption in intestine) • Chief cells secrete pepsinogen (precursor for pepsin) 18-29
HCl in Stomach • Is produced by parietal cells which pump H+ into lumen via an H+/ K+ pump (pH ~1) • Cl- is secreted by facilitated diffusion • H+ comes from dissociation of H2CO3 • Cl- comes from blood side of cell in exchange for HCO3- 18-31
HCl in Stomach continued • Is secreted in response to the hormone gastrin; and ACh from vagus • These are indirect effects since both stimulate release of histamine which causes parietal cells to secrete HCl 18-32
HCl in Stomach continued • Makes gastric juice very acidic which denatures proteins to make them more digestible • Converts pepsinogen into pepsin • Pepsin is more active at low pHs 18-33
Protection of Stomach Against HCL and Pepsin • Both HCL and pepsin can damage lining and produce a peptic ulcer • 1st line of defense is the adherent layer of mucus • = a stable gel of mucus coating the gastric epithelium • Contains bicarbonate for neutralizing HCL • Is a barrier to actions of pepsin • Gastric epithelial cells contain tight junctions to prevent HCL and pepsin from penetrating the surface • Gastric epithelial cells are replaced every 3 days 18-34
Digestion and Absorption in Stomach • Proteins are partially digested by pepsin • Carbohydrate digestion by salivary amylase is soon inactivated by acidity • Alcohol and aspirin are the only commonly ingested substances that are absorbed 18-35
Gastric and Peptic Ulcers • Peptic ulcers are erosions of mucous membranes of stomach or duodenum caused by action of HCl • In Zollinger-Ellison syndrome, duodenal ulcers result from excessive gastric acid in response to high levels of gastrin • Helicobacter pylori infection is associated with ulcers • Antibiotics are useful in treating ulcers • And also proton pump inhibitors such as Prilosec • Acute gastritis is an inflammation that results in acid damage due to histamine released by inflammation • Is why histamine receptor blockers such as Tagamet and Zantac can treat gastritis 18-36
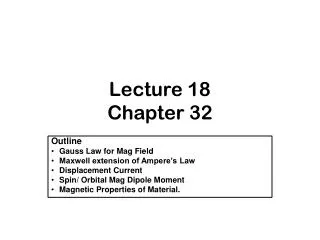
Vertical banded gastroplasty http://www.nlm.nih.gov/medlineplus/ency/imagepages/19498.htm
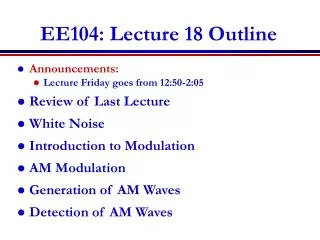
Lap Band procedure http://www.weight-loss-i.com/gastrointestinal-weight-surgery.htm
Small Intestine 18-37
Small Intestine (SI) • Is longest part of GI tract; approximately 3m long • Duodenum is 1st 25cm after pyloric sphincter • Jejunum is next 2/5 of length • Ileum is last 3/5 of length; empties into large intestine 18-38
Small Intestine (SI) continued • Absorption of digested food occurs in SI • Facilitated by long length and tremendous surface area 18-39
Small Intestine (SI) continued • Surface area increased by foldings and projections • Large folds are plicae circulares • Microscopic finger-like projections are villi • Apical hair-like projections are microvilli 18-40
Small Intestine (SI) continued • Each villus is covered with columnar epithelial cells interspersed with goblet cells • Epithelial cells at tips of villi are exfoliated and replaced by mitosis in crypts of Lieberkuhn • Inside each villus are lymphocytes, capillaries, and central lacteal 18-41
Small Intestine (SI) continued • A carpet of hair-like microvilli project from apical surface of each epithelial cell • Create a brush border 18-42
Intestinal Contractions and Motility • 2 major types of contractions occur in SI: • Peristalsis is weak and slow and occurs mostly because pressure at pyloric end is greater than at distal end • Segmentation is major contractile activity of SI • Is contraction of circular smooth muscle to mix chyme (shown in diagram) 18-44
Large Intestine 18-48
Large Intestine (LI) or Colon • Has no digestive function but absorbs H2O, electrolytes, B and K vitamins, and folic acid • Internal surface has no villi or crypts and is not very elaborate • Contains large population of microflora • = 1013 to 1014commensal bacteria of 400 species • which produce folic acid and vitamin K and ferment indigestible food to produce fatty acids • And reduce ability of pathogenic bacteria to infect LI • antibiotics can negatively affect commensals 18-49
Large Intestine (LI) or Colon continued • Extends from ileocecal valve at end of SI to anus • Outer surface bulges to form pouches (haustra) 18-50
Fluid and Electrolyte Absorption in LI • SI absorbs most water but LI absorbs 90% of water it receives • Begins with osmotic gradient set up by Na+/K+ pumps • Water follows by osmosis • Salt and water reabsorption stimulated by aldosterone • LI can also secrete H2O via active transport of NaCl into intestinal lumen 18-51
Liver 18-53
Structure of Liver • Liver is the largest internal organ • Hepatocytes form hepatic plates that are 1–2 cells thick • Plates are separated by sinusoids which are fenestrated and permeable even to proteins • Contain phagocytic Kupffer cells 18-54
Structure of Liver continued • A damaged liver can regenerate itself from mitosis of surviving hepatocytes • In some cases, such as alcohol abuse or viral hepatitis, regeneration does not occur • Can lead to liver fibrosis and ultimately cirrhosis 18-55
Hepatic Portal System • Food absorbed in SI is delivered 1st to liver • Capillaries in digestive tract drain into the hepatic portal vein which carries blood to liver • Hepatic vein drains liver • Liver also receives blood from the hepatic artery 18-56
Liver Lobules • Are functional units formed by hepatic plates • In middle of each is central vein • At edge of each lobule are branches of hepatic portal vein and artery which open into sinusoids 18-57