Download
1 / 54
540 likes | 692 Views
Nursing Care Plan of Aortic Aneurysm. An-Najah National University Faculty of Nursing Second year students Prepared by: Abed Alaziz Al Masri Obiedah Nasfat Abed Elsalam Isa. What is Aortic Aneurysm ?.

E N D
Nursing Care Plan of Aortic Aneurysm An-Najah National University Faculty of Nursing Second year students Prepared by: Abed Alaziz Al Masri ObiedahNasfat Abed Elsalam Isa
What is Aortic Aneurysm ? • Is a localized sac or dilation at a weak point of the aorta to a size greater than 1.5 times its normal diameter
What are the causes of Aortic Aneurysm? • Most aneurysms are arteriosclerotic in origin • Syphilis • Infection • Inflammatory diseases • Trauma • Hypertension • Smoking • Aortic dissection
What are the classifications of aneurysms according to their shape ? • The first classification is : • Fusiform Aneurysm : dilation of the entire circumference of the artery • Saccular Aneurysm : localized balloon- shaped outpouching projects from one side of the artery
The second classification is : • True Aneurysm : involve the entire vessel wall • False Aneurysm : is formed when blood leaks outside of the artery but is contained by the surrounding tissues • A pseudoaneurysm, or false aneurysm, is an enlargement of only the outer layer of the blood vessel wall • A false aneurysm may be the result of a prior surgery or trauma
Thoracic Aortic Aneurysm (TAA) • Occur most frequently in men between the ages 40 and 70 years • About one third of patients with (TAA) die of rupture of the aneurysm
Thorasic Aorta Aneurysm- Clinical manifestations • Back, neck or substernal pain • Dyspnea, stridor or brassy cough if pressing on trachea • Hoarseness • Edema of the face and neck • Distended neck vein • Aphonia • Disphagia • Complications: such as rupture and hemorrhage
What are the diagnostic tests for (TAA) ? Chest x-ray Computed tomography (CT) Transesophagial echocardiography
Abdominal Aortic Aneurysm (AAA) • Affects men four times more often than women and is most prevalent in elderly patients • Most of these aneurysms occur below renal arteries (infrarenal aneurysm) • Untreated, the eventual outcome may be rupture and death
Clinical manifestations of (AAA) • Patients with (AAA) feel their heart beating in their abdomen when lying down • Client´s awareness of a pulsating mass in the abdomen, with or without pain, followed by abdominal pain and back pain • Flank pain or groin pain may be experienced because of increasing pressure on other structures sometimes mottling of the extrimities or distal emboli in the feet alert the clinician to a source in the abdomen
Clinical manifestations of (AAA) • Aortic calcification noted on x-ray • Mild to severe midabdominal or lumbar back pain • Cool, cyanotic extrimities if iliac arteries are involved • Claudication (ischemic pain with exercise, relieved by rest) • Complication: peripheral emboli to lower extrimities • Rupture and hemorrage
Who’s at risk? • In 20% of patients, familial clustering of aortic aneurysms suggests a hereditary tendency to develop aneurysms, aortic aneurysms also can be an individual aberration present at birth • Pregnancy can hasten aneurysm development because of hormonal and hemodynamic changes
Other risk factors include a history of Smoking Chronic obstructive pulmonary disease Hyperlipidemia Poorly controlled diabetes Connective tissue disorders, including Marfan syndrome (which is a genetic connective tissue disorder that affects the skeleton, eyes, and cardiovascular system) Mycotic aneurysms, develop from streptococcal, staphylococcal, or salmonella infections of the aorta
Indications for Surgical Repair of Aortic Aneurysms Thoracic Diameter 6 cm (5 cm in patients with Marfan syndrome) Symptoms suggesting expansion or compression of surrounding structures Abdominal Diameter 5 cm or more Diameter 4 cm or less, need regular follow-up Diameter 4–5 cm, management is controversial Others Rapidly expanding aneurysms (growth rate > 0.5 cm over a 6-month period) Symptomatic aneurysm regardless of size
Implement Interventions to Reduce the Risk of Aneurysm Rupture • Maintain bed rest with legs flat • Maintain a calm environment, implementing measures to reduce psychologic stress • Prevent straining during deafecation • Administer beta blockers and antihypertensive as prescibed • Elevating or crossing the legs restricts peripheral blood flow and increases pressure in the aorta or iliac arteries
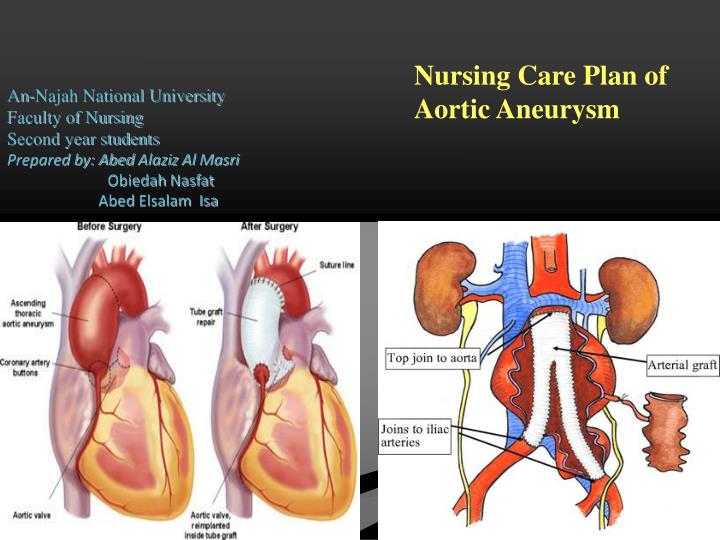
Abdominal Aortic Aneurysm- Open Repair • Open repair of an abdominal aortic aneurysm involves an incision of the abdomen to directly visualize the aortic aneurysm • The procedure is performed in an operating room under general anesthesia • The surgeon will make an incision in the abdomen either lengthwise from below the breastbone to just below the navel or across the abdomen and down the center
Abdominal Aortic Aneurysm- Open Repair • The aneurysm is exposed, the aorta is clamped just above and below the aneurysm to stop the flow of blood, the aneurysm is opened and a Dacron graft is placed within the anuerysm • The aneurysm sac is then wrapped around the graft to protect it
Open Repair • The graft is sutured to the aorta connecting one end of the aorta at the site of the aneurysm to the other end of the aorta • Open repair remains the standard procedure for an abdominal aortic aneurysm repair
Endovascular Aneurysm Repair (EVAR( • EVAR is a minimally-invasive (without a large abdominal incision) procedure performed to repair an abdominal aortic aneurysm • EVAR may be performed in an operating room, radiology department, or a catheterization laboratory • The physician may use general anesthesia or regional anesthesia (epidural or spinal anesthesia) • The physician will make a small incision in each groin to visualize the femoral arteries in each leg
Endovascular Aneurysm Repair (EVAR) • With the use of special endovascular instruments, along with x-ray images for guidance, a stent-graft will be inserted through the femoral artery and advanced up into the aorta to the site of the aneurysm
Endovascular Aneurysm Repair (EVAR( • A stent-graft is a long cylinder-like tube made of a thin metal framework (stent). The stent helps to hold the graft in place • The stent-graft is inserted into the aorta in a collapsed position and placed at the aneurysm site • Once in place, the stent-graft will be expanded (in a spring-like fashion), attaching to the wall of the aorta to support the wall of the aorta • The aneurysm will eventually shrink down onto the stent-graft
Risks of the Procedure- open repair Myocardial infarction Irregular heart rhythms Bleeding during or after surgery Injury to the bowel Limb ischemia Embolus to other parts of the body Infection of the graft Lung problems Kidney damage Spinal cord injury Damage to surrounding blood vessels, organs, or other structures by instruments Groin wound infection Groin hematoma Endoleak Allergy
Nursing Assessment • Attention to the character and quality of the peripheral pulses and the neurologic status • Pedal pulse sites (dorsalis pedis and posterial tibial) and skin lesions on the lower Extrimities should be marked and documented before surgery
Planning • The overall goals for a patient undergoing aortic surgery include: • Normal tissue perfusion • Intact motor and sensory function • No complications related to surgical repair such as thrombosis or infection
Nursing Implementation- Graft Patency • Maintain adequate blood pressure to promote graft patency. Prolonged hypotention may result in graft thrombosis due to decreased blood flow • Administration of of i.v. fluids and blood components as indicated is essential to maintaining adequate blood flow to the graft • Central venous pressure readings or pulmonary artery pressures and urinary output should be monitored hourly in the immediate postoperative period to help assess the patient´s state of hydration
Nursing Implementation- Graft Patency • Severe hypertention may cause undue stress on the arterial anastomosis resulting in leakage blood or rupture at the suture lines • Drug therapy with duiretics or i.v antihypertensive agents may be indicated if severe hypertension persists
Nursing Implementation- Cardiovascular Status • In individuals with preexisting coronary artery disease, myocardial ischemia or infarction may occur in the perioperative period due to decreased oxygen supply to the heart or increased oxygen demands on the heart. Cardiac rhythmias also may occur due to electrolyte imbalances, hypoxemia, hypothermia or myocardial ischemia • Nursing interventions include continous ECG monitoring, frequent electrolyte and blood gas (ABG) determinations, administrations of oxygen and antiarrhythmic medications as needed • Replacement of electrolytes as indicated, adequate pain control and resumption of preoperative cardiac medications
Infection Diagnosis Risk for infection related to presence of a prosthetic vascular graft and invasive lines Outcome Normal body temperature No signs of infection Wound is well approximated
Nursing Implementation- Infection • Nursing prevention to prevent infection should include ensuring that the patients receives a broad spectrum antibiotic as prescribed • Monitor for signs of infetion • The nurse should ensure adequate nutrition and observe the surgical incision for any evidence of delaying healing or prolonged drainage
Nursing Implementation- Infection • All i.v., arterial and central venous catheter insertion sites should be carried for carefully with the use of sterile technique because they are frequently a portal of entry for bacteria • Meticulous perianial care for the patient withan indwelling urinary catheter is essential to minimize the risk of urinary tract infection • Surgical incisions should be kept clean and dry
Nursing Implementation- Gastrointestinal Status • Paralytc ileus may develop as a result of anesthesia and the manual manipulation and displacement of the bowel for long periods during surgery • The intestine may become swollen and bruised and pristalsis ceases for variable intervals • A nasogastric tube is inserted during surgery and connected to low, intermittent suction • This decompreses the stomach and duodenum, prevent aspiration of stomch contents, and decrease pressure on suture lines
Nursing Implementation- Gastrointestinal Status • The nasogastric tube should be irrigated with normal saline solution as needed and the amount and character of the drainage should be recorded • The nurse should auscultate for the return of bowel sounds • The passing of the flatus is a key sign of returning bowel function and shoud be noted • Early ambulation will assist with the resumption of bowel functioning • It is unusual for paralytic ileus to persist beyond the fourth postoperative day
Diagnose: risk for ischemia of the bowel • If the client undergoes extensive aortic procedures that involve clamping the mesenteric vessels, ischemic colitis can develop • Inferior mesenteric artery can embolize • The lack of blood supply can lead to ischemia and ileus Outcomes • The nurse will monitor the client for abdominal distention, diarrhea, severe abdominal pain, sudden elevation in white blood cell count and bowel sound
Intervention • Assess bowel sounds every 4 hours • Keep the client NPO and provide oral care every 2-4 hr • Provide routine nasogastric tube care and assess nares for tissue impairment • Perform guaiag test (Test for blood in stool) of NG drainage every 4 hours or if bleeding is suspected (i.e., drainage has dark, coffee-ground appearance or is bright red) 36
Nursing Implementation- Neurologic Status • When the ascending aorta and aortic arch are involved, nursing interventions should include: • assessment of level of conciosness, pupil size and response to light, facial symmetry, tongue deviation, speech, ability to move upper extrimities, quality of hand grasps, • the carotid, radial, and temporal artery pulses should be assessed • When the descending aorta is involved, nursing assessment of: • the ability to move lower extrimities • pulses to be assessed may include the femoral, popliteal, posterior tibial and dorsalis pedis
Nursing Implementation- Peripheral Perfusion Status • When checking the pulses, the nurse should mark the locations lightly with a felt-tip pen so that others can locate them easily • An ultrasonic Doppleris useful in assessment of peripheral pulses • It is also important to note the skin temperature and color, capillary refill time and sensation and movement of the extrimities
Nursing Implementation- Peripheral Perfusion Status • A decreased or absent pulse in conjunction with a cool, pale, mottled or painful extrimity may indicate embolization of aneurysmal thrombus or plaque or occlusion of the graft • Gaft occlusion is treated with reoperation if identified early • In rare instances, thrombolytic therapy may also be considered
Nursing Implementation- Renal Perfusion Status • One of the causes of decreased renal perfusion is embolization of a fragment of thrombus or plaque from the aorta that subsequently lodges in one or both of the renal arteries • This can cause ischemia of one or both kidneys • Hypotension, dehydration, prolonged aortic clamping, or blood loss can also lead to decreased renal perfusion
Nursing Implementation- Renal Perfusion Status • The patient return from surgery with an indwelling urinary catheter in place • An accurate record of fluid intake and urinary out- put should be kept until the patient resumes the preoperative diet • Daily weight also should be obtained • Central venous pressure reading and pulmonary artery pressures also provide important information regarding hydration status
Diagnose • Risk for hemorrhage because of the risk of bleeding at the graft site, the client is at risk for hemorrhage • Risk for deficient fluid volume Outcome • The nurse will monitor for manifestations of hemorrhage and notify the physician if any manifestations occur
Interventions- Monitor the client for: increase in pulse rate decrease in blood pressure clammy skin pallor anxiety & restlessness decreasing levels of conciousness Cyanosis thirst oliguria increase abdominal girth increased chest tube output greater than 100 ml/hr/for 3 hours back pain from retroperitoneal bleeding
Diagnose Risk for impaired gas exchange • Impaired gas exchange related to ineffective cough secondary to pain from large incision Outcome • The client will have improved gas exchange as evidenced by oxygen saturation or Pao2 greater than 95%, increasing effectiveness in coughing, and clearing of lung sounds
Intervention Monitor settings on ventilator to ensure the client is adequately oxygenated Assess lung sounds every 1 to 2 hours Monitor oxygen saturation continously. Report any desaturation After extubation, assist with coughing by using incentives spirometry, provide splinting pillows before coughing, encourage ambulation provide adequate analgesia Spirometry
Diagnose • Risk for inadequate tissue perfusion • During the operation, aorta is clamped to stop bleeding while the graft is placed • During that time, peripheral tissues are not perfused • The graft site can also become occluded with thrombus • In addition the client often has preexisting arterial disease Outcomes • The client will maintain adequate tissue perfusion as evidenced by: • pedal pulses • warm feet • capillary refill of less than 5 seconds, • abscence of numbness or tingling • ability to dorsiflex and plantar flex both feet equally • Urin output adequate
Plantar Flexion • Extension of the ankle resulting in the forefoot moving away from the body. • Dorsal Flexion • Flexion of the ankle resulting in the top of the foot moving toward the body
InterventionRisk for Inadequate Tissue Perfusion • Administer i.v. Fluid at prescribed rates to ensure adequate hydration and renal perfusion • Maintain a warm environment to prevent temperature induced vasoconstriction • Administer anticoagulants and /or antiplatelet agents as prescribed to prevent thrombus formation • Monitor urinry output daily weights, BUN, and serum createnine to detect signs of altered perfusion and renal failure
Acute Pain Diagnosis: • Acute pain related to surgical incision Outcomes • The client will have increased comfort as evidenced by : • self-report of decreasing levels of pain • use of decreasing amounts of opioid analgesics for pain control • ambulating or coughing without extreme pain 49
Intervention • Opioids are usually provided via a patient-controlled analgesia system or through an epidural catheter • Asses the degree of pain often and record the baseline level of pain and the degree to which pain is reduced by medications or other intervention • When changing to an oral route for pain management, plan to pretreat the pain with oral medications 30 minutes or more before discontinuing the infusion 50