Download
1 / 36
490 likes | 1.34k Views
AIRTRAQ LARYNGOSCOPE. February 2007. Click to continue. Airtraq Optical Laryngoscope. Index. Introduction to Airway Management Airtraq Features & Design Characteristics Clinical Experience & Feedback Instructions for Use / Tips / Airtraq Sizes Video System description

E N D
AIRTRAQ LARYNGOSCOPE February 2007 Click to continue
Airtraq Optical Laryngoscope Index • Introduction to Airway Management • Airtraq Features & Design Characteristics • Clinical Experience & Feedback • Instructions for Use / Tips / Airtraq Sizes • Video System description • Distribution. Present status. • Training Material • When and where to use it. Alternative devices. • How to start using the Airtraq • Manekin Practice Click to continue
Glottis Anatomy Epiglottis Vocal cords Arytenoids Esophagus
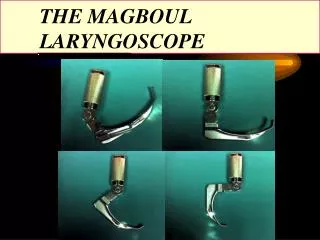
Direct Laringoscopy Macintosh blade Miller blade
Airtraq Features • Airtraq is a new intubation device, developed, and patented by Dr. Acha. It offers: • Full visualization of the airway, during 100% of the laryngoscopic procedure, facilitating tracheal intubation and avoiding esophageal and bronchial intubations • No hyperextension of the neck required • Allows intubation of patients in any position, e.g., sitting, allowing the clinician optimal access with respect to the patient • Easy to use • Short learning cycle • Versatile. Broad field of applications. Click to next page
Airtraq Design Characteristics • Anatomically shaped • High quality optical system in separate visualization channel • Guide channel for insertion of the endotracheal tube • Anti-fog system for optics • Light source ( low temperature ) for illuminating the anatomy • Single use device • Uses any standard endotracheal tube • Two sizes (plus paediatric in 2008). • Available clip-on video system to allow viewing on an external screen Click to next page
Airtraq Detailed Description 1 3 7 7 3 5 4 2 1. Viewfinder 2. Optical Duct 3. Rubber Viewfinder 4. ET Channel 5. Battery box 6. Light (LED) 7. Switch 8. Anti-fog system 8 6
Optics and View • Developed with Spanish Navy – eye glass quality, but disposable
Glottis Optics ETT Viewer The “View” • Optics and guiding channel “point” the user to the center of the viewing window. • The user only has to center the vocal cords in the middle of the image and the ETT goes in.
Airtraq LaryngoscopeClinical Testing through January 2007 • More than 5,000 succesful intubations • All Cormack III and IV patients became Cormack I, II using the Airtraq • Male and female from 36 kg to over 150 kg all intubated with the regular size • Morbidly obese patients • Intubations without muscle relaxants • Frontal intubations with patient in the upright and sitting position • Intubations of awake patients • Emergency intubations of severely injured patients Click to next page
Results 1st Study - University of Ireland Results. The Airtraq® proved easy to learn and performed similarly to the Macintosh laryngoscope in the normal airway. Initially, tracheal intubation of the normal airway took significantly longer with the Airtraq device, but this was eliminated at the end of the protocol, illustrating a steep learning curve. In simulated difficult airway scenarios, the Airtraq® proved easier to use, resulted in less dental trauma, and had greater success in tracheal intubation than the Macintosh Laryngoscope. Conclusions. This manikin study demonstrates that the Airtraq® performs comparably to the Macintosh laryngoscope in the normal airway, when used by experienced anaesthetists. The Airtraq® appears to hold particular promise for the management of the difficult airway.
Airtraq – Feedback from Anesthesiologists • T. N., MD, FACEP. Associate Residency Director. USA University: • “I had the opportunity to use the Airtraq - a potentially difficult airway - obese endstage liver and renal dz. Intubation was very smooth, quick visualization and then was able to ventilate while watching the tube position during removal. I'd love to get more of these - and really love to get the camera!” • N. G., MD, Univ. Graduate Research Professor USA University • “You can add me to the list of people who are airtraq coverts. last night had a mal 1 airway , small chin, great opening, able to bite upper lip, normal dentition. Couldn’t visualize with either mac or miller [blade] attempts. I got an air traq from my locker and a novice used it and it passed what I call the "oh wow" test. Both residents were impressed as was I. It was my first unexpected difficult airway where I have put the device to good use.”
Airtraq – Feedback from Anesthesiologists • Dr. M.W., FRCA Consultant Anaesthetist , UK Major Hospital • “I am sure that the Airtraq device is going to be a great success and hope that I will be able to be associated with the product” • Dr. C. M., Consultant Anaesthetist , Ireland. • “Yesterday, I did a nasal intubation on an adult, handicapped patient with a documented difficult airway. I could not blindly pass the ETT through the nose, so I had to use the Macintosh laryngoscope. Well, she was a Mallampatti grade IV and a Cormac-Lehane grade IV. I could not see a thing with the Macintosh - not even the epiglottis. Well, with the Airtraq, it simply and smoothly gave me a grade I Cormac-Lehane view. I did not have to use any force or upward lifting manoeuvres whatsoever. The Airtraq then guided me in the placement of the nasal tube - no problem at all !! Again, this reinforces how amazing this device is”
Airtraq – Feedback • S.H., Intensive Care Paramedic , Australia: • I've just used the Airtraq (regular size) successfully in the field on a difficult airway, 12 year child hit by a car, severe trauma, cervical spine immobilisation, funny mouth and teeth, the tube went in first attempt with the Airtraq, great visualisation and very reassuring to actually see the tube in there and to be able to go back and check with that great view of everything glottic.
5. Airtraq Laryngoscope -Instructions for Use I. PREPARATION • Turn ON the light. Wait until the light stops blinking • Lubricate the ET tube and place it into the lateral channel with its tip aligned with the end of the lateral channel of the Airtraq II. AIRTRAQ PLACEMENT • Insert the Airtraq into the midline of the patient´s mouth, taking care to keep aside the tongue so that it does not falls into the mouth • Slide the Airtraq through the oropharynx and larynx, keeping it in the midline • Look through the eyepiece to view the airway and to identify structures • Continue insertion until you see the epiglotis and the vocal cords III. ET Tube INSERTION • Advance the ET Tube by pushing it until you see the ET tube as it passes through the vocal cords • Verify ET tube placement and insertion length. • Inflate the ET tube cuff, connect the ET tube to the breathing circuit and verify placement and seal. IV. AIRTRAQ EXTRACTION • Separate the ET tube from the Airtraq by pulling it laterally. Make sure to hold ET tube while sliding the Airtraq backwards. • Make sure that the ET tube has not moved and remains properly positioned.
Tips to maximize AIRTRAQ effectiveness. • Insert and slide the Airtraq softly and slowly. • Keep the tongue aside • Always keep the Airtraq on the mouth´s midline. • In case structures (arytenoids, epiglottis, etc.) are not recognized, WITHDRAW theAirtraq slightly. • Do not introduce the Airtraq too deep. If the ETT hits the arytenoids, epiglottis or goes to the esophagus WITHDRAW the Airtraq by rotating it back. • Once the tip is located in the vallecula, gently LIFT UP the Airtraq (do not tilt or use a lever action). • To expose the vocal cords, the tip of the Airtraq can be located either in the vallecula (Macintosh style), or under the epiglottis (Miller style). • TWIST the Airtraq to CENTRE the vocal cords in the image. • Advance the ETT slowly without twisting it. • In case the ETT hits the arytenoids withdraw slightly the Airtraq and advance gently again the ETT.
How to select the appropiate Airtraq • Works with any type of ETT • Standard • Reinforced (wired) • Pre-shaped • Regular Size : Minimum mouth opening 18 mm • Can fit patients from 40 kg to 200 kg. • Can be used always that the mouth can open up to two fingers. • ETT sizes: 8.5 / 8.0 / 7.5 /7.0 (6.5/6.0) Up to 8.5 • Small Size : Minimum mouth opening 16 mm • First Choice for small adults or adolescents. Can fit patients from 25 kg to 100 kg. • ETT sizes: 7.5 / 7.0 / 6.5 / 6.0 Up to 7.5
Airtraq – Video System • Perfect for teaching and training • Works as an optional accessory for the Airtraq • Reusable. Wireless or wired operation. • It should be mounted on top of the Airtraq after removing the original rubber viewfinder (a simple and quick operation) • The Video System has to main devices: • Clip-on Camera (can be connected through a cable to any monitor) • Camera: with rechargeable Li-Ion Battery and wireless 2.4 GHz emitter. • Video Cable: to connect the Camera to an external monitor. • RCA / BCN Adaptor :needed to connect to most monitors in OR • Camera stand-alone battery charger • Wireless Receiver (optional) • Wireless Receiver: 2.4 GHz Receiver with rechargeable Li-Ion battery and a battery charger that can recharge the batteries of both Receiver and camera. • Camera Battery Charge Cable: to charge the Li-Ion Battery of the Camera from the Receiver • Power Cable • Allows to record the images into a laptop or DVD recorder.
Airtraq – Training material • Brochure • Videos • DVD • Web Site www.airtraq.com • Email airtraq@prodolmed.com
Countries where the Airtraq is used • America: • USA • Canada • Argentina • Chile • Venezuela • Perú • Others : • Japan • Korea • Australia • New Zealand • Saudi Arabia • Kuwait • United Emirates • Europe : • Germany • France • UK • Italy • Spain • Netherlands • Belgium • Switzerland • Austria • Ireland • Finland • Portugal • Eslovenia
Airtraq – When and where to use it “Challenging” intubations Any anticipated difficult airway Unanticipated Cormack III and IV patients Infectious patients Obese patients Cervical Trauma Other uses • Emergency settings • Cervical spine immobilization • ICU ET tube exchange • Double lumen ETT Intubation • Nasotracheal Intubations • Fibroscope and Gastroscope guidance
Alternative devices DeviceDisadvantages Glidescope Reusable , Requires investment , Does not guide the ETT, Usually needs some hyperextension, Needs Set up LMA Blind, No intubation, risk of bronchoaspiration Fastrack Blind intubation, Reusable, Slow learning curve, needs special ETT C-Trach Reusable, Requires investment , ETT blocks vocal cords view Poor quality image, Needs set up, Slow learning curve, Needs special ETT Mcgrath Requires investment , Does not guide the ETT, No anti fog system. Needs some hyperextension, Small scrren. Fibroscope Requires investment , Reusable, Needs continuos training, Slow learning curve, Requires Set up, Clening and maintenence costs. Upsher, etc Reusable, Requires investment , Fiberoptics parallel to ETT trajectory
How to start using the Airtraq • Read instructions for use • View videos • Review tips for effectiveness. • Remenber that most of first users tend to introduce the Airtraq too deep inside. • Always lift up the Airtraq to obtain a full exposure of the Airtraq • If possible intubate a manekin • Try to use the Video System for the initial intubations. • Start with easy airway patients
Manekin practice • Most manekins do not replicate well the Airway anatomy. • There are special Demo Airtraqs in order to work in manekins. The antifog system is deactivated so that the batteries last longer. • Exercises with manekin • Introduce the Airtraq and look before it gets vertical. Keep advancing while looking through the viewfinder • Withdraw and advance the Airtraq while looking. • Place the blade of the airtraq in the vallecula and under the epiglottis • Advance and withdraw the ETT. • Advance the ETT and pinge both arytenoids by twisting the Airtraq clock and anticlokwise. • Withdraw the Airtraq slightly and see how the ETT avoids the arytenoids and aligns with the vocal cords.