Download
1 / 46
470 likes | 600 Views
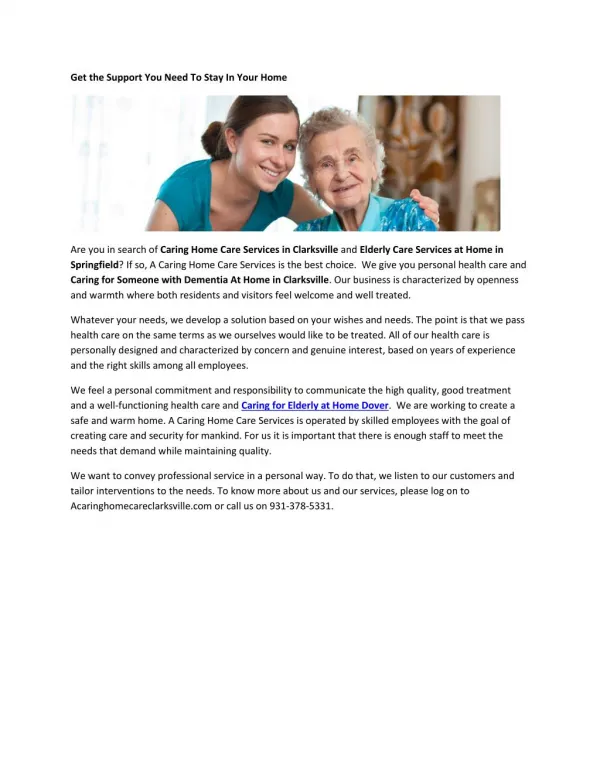
Special Concerns in Caring for the Elderly Adult. Pain Management Violence and Elder Mistreatment. Scenario…. S. T. is a 68 year old female who comes alone to your E.R.. She complains of shortness of breath. Vitals: Ht. 65” Wt. 101 lbs BP 155/84 Pulse 88

E N D
Special Concerns in Caring for the Elderly Adult Pain Management Violence and Elder Mistreatment
Scenario…. • S. T. is a 68 year old female who comes alone to your E.R.. • She complains of shortness of breath. • Vitals: Ht. 65” Wt. 101 lbs BP 155/84 Pulse 88 • When electrodes are placed for an EKG, you notice bruising across her chest. • Her son comes in and states, “You fell down the stairs, again, didn’t you, Mom?”
What is pain? • Pain is an unpleasant feeling often caused by noxious or injurious stimuli • Pain usually prompts the person to withdraw from the cause of the pain and avoid it in the future • Most pain resolves promptly once the cause is removed • Other types of pain continue (chronic) • At times pain occurs without any recognizable cause • In the United States, pain complaints prompt the majority of all doctor visits • Pain is costly • Pain can negatively affect a person's quality of life • Psychological and social factors can affect the nature of pain
Persistent pain in the elderly is associated with… • Functional impairment • Falls • Slow rehabilitation • Depression • Anxiety • Decreased socialization • Sleep disturbance • Increased healthcare utilization and costs • The Joint Commission on Accreditation of Healthcare Organizations has mandated pain screening noting pain “the fifth vital sign.”
Importance in the care of the elderly • Painful conditions are common in this population • Undertreatment is common • Patients with dementia may not express pain effectively • Fear of “addiction” is common • Some believe unrelieved pain is to be expected • Lack of routine pain assessment • Ineffective methods of assessment
Duration of pain • Acute pain—resolves quickly • Chronic pain definition is arbitrary… • More than 30 days • 3 months • 6 months • Some say the transition from acute to chronic pain occurs at 12 months • Chronic pain is sometimes classified as: • Cancer pain, or, • Benign pain
Nocioceptive pain • Nocioceptors are nerve cell endings that initiate the sensation of pain • They respond to stimuli that threaten to cause harm to the individual • Examples are • Heat • Cold • Crushing or tearing • Chemical injury
Neuropathic • Pain caused by injury to the nervous system itself • Described as • Burning • Tingling • Electrical • Stabbing • Pins and needles
Phantom pain • Pain experience a part of the body that is no longer • Type of neuropathic pain • Common in amputee patients
Psychogenic pain • Pain affected by • Mental, • Emotional, • Behavioral factors • Sometimes include specific situations with no other identifiable cause… • Headache • Back pain • Stomach pain
Breakthrough pain • Pain that “breaks through” a patient’s normal pain management dosing • Comes on suddenly • Common in patients managed for cancer pain • Alternating pain medicine dosing sometimes helpful
Incident pain • Episodic increase in pain intensity • Can come from a specific activity • Or, not related to any activity • Arthritic joint • Bumping an injured site
Acute pain in older adults • Similar to acute pain in other populations • Also due to exacerbations of chronic conditions • Situations to which they are more at risk: • UTI • Decubitus ulcers • Pneumonia • Constipation • Injury due to diminished protective mechanisms
Chronic pain in older adults • 1 in 5 patients age 65 or older • Generally lasting >3-6 months • All are candidates for pharmacological therapy • Exacerbated by depression • Can create a vicious cycle
Pain causes among older adults • Osteoarthritis and rheumatoid arthritis • Spinal stenosis • Peripheral neuropathy • Post-herpetic neuralgia • Fibromyalgia • GERD • Peripheral vascular disease • Headache • Post-surgical pain • Pressure ulcers • Angina, cardiac disease • Cancer pain, pain of treatment
Assessing pain in the older adult • Pain intensity (0-10) • Pain frequency • Pain location (use the “one finger” rule) • Duration • What makes it better? • What makes it worse? • What are the effects on his or her functional level? • Continue to assess until acceptable level of relief has been achieved • Assessment must be documented to be complete
Special cases…the patient with dementia • Need to rely on cues other than verbal communication, including… • Facial expression • Vocalizations • Body movements • Change in person-person interaction • Change in activity patterns • Mental status changes
Pain management plans • Include both acute and chronic pain • Include both pharmacological and nonpharmacological interventions • Must be individualized • Must be titrated, i.e., provided based on the level of pain reported or the level of pain assessed if the patient is nonverbal • Start with smaller doses to avoid toxicity • Consider oral route first • Often involves “rational polypharmacy” • 2 or more drugs in combination with • Complementary therapy
Opioid use in the older adult • Great efficacy in moderate to severe pain • No maximum dose • Can be used for long periods of time • Minimal organ damage • Some are inappropriate for the elderly adult: Meperidine—confusion, seizures Propoxyphene—delirium, ataxia, dizziness (withdrawn)
Adverse side effects of opioids • Constipation • Sedation • Respiratory depression • Nausea and vomiting • Myoclonus • Pruritis
Considerations in opioid use • Titrate slowly • Bowel regimen to prevent constipation • Watch for signs of sedation and protect patient • Monitor for respiratory depression, provide O2 if necessary • Antiemetics for nausea/vomiting • Use antihistamines cautiously for pruritis
Definition of elder abuse • The physical or psychologic mistreatment, neglect, or financial exploitation of the elderly.” • Several types of abuse are common • Each type may be intentional or unintentional • Perpetrators are usually spouses or adult children • May be other family members • Paid or informal caregivers
Physical abuse • “The use of force that results in physical or psychological injury.” • Includes striking, shoving, shaking, beating, restraining and improper feeding • May include sexual assault, i.e., any form of sexual intimacy without consent or by force or threat of force
Psychologic abuse • The use of words, acts, other means that cause emotional stress or anguish • Includes threats (e.g. of institutionalization), insults and harsh commands • Remaining silent • Ignoring the person • Infantilization: encouraging the victim to become dependent on the abuser
Neglect • Failing to provide essentials • Food • Medicine • Personal care
Financial abuse • The exploitation of or inattention to a person’s possessions or funds • Includes swindling • Pressuring a person to distribute assets • Managing a person’s money irresponsibly
Healthcare fraud and abuse • Duplicate billings for the same medical service or device • Evidence of overmedication or undermedication • Evidence of inadequate care when bills are paid in full • Problems with a care facility • Poorly trained, poorly paid or insufficient staff • Crowding • Inadequate responses to questions about care
Epidemiology of elder abuse • True incidence is unclear • Appears to be a growing public problem in the USA • One large study showed 3.2% of individuals ≥ 65 years were victims of physical abuse, psychologic abuse or neglect • Study did not include financial abuse
Risk factors for elder abuse (1) • Chronic disease and or functional impairment of the victim • The elder person’s ability to escape, seek help and defend himself is reduced • Social isolation of the victim • Abuse of isolated persons is less likely to be detected and stopped • Cognitive impairment • Persons with dementia may act aggressively and disruptively, precipitating abuse
Risk factors for elder abuse (2) • Substance abuse • Alcohol or drug abuse • Psychiatric disorder • Schizophrenia, other psychoses • Patients discharged from an inpatient facility may return to their elder parents’ home for care • These younger patients may become violent at once at home • History of violence • History of violence in a relationship and outside the family may predict abuse • Violence is a learned response to life challenges
Risk factors for elder abuse (3) • Dependence of abuser on victim • Financial support, housing, emotional support • Family member’s attempts to obtain resources from elderly person can result in abuse • Dependence can produce resentment • Stress affecting abuser • Chronic financial problems • Death in the family • Responsibilities of caregiving • Shared living arrangements • Opportunities for tension and conflict are greater
Difficulty of diagnosis • Many signs are subtle • Victim often unwilling or unable to discuss the abuse • Shame • Fear of retaliation • Desire to protect the abuser
Failure of healthcare • “Ageist” response from nurses, doctors, others • Dismiss complaints of abuse as: • Confusion • Paranoia • Dementia
Social isolation and identification of abuse • Abuse tends to increase the isolation • Abuse limits the victim’s access to the outside world • Denies visitors • Refuses telephone calls
Obtaining the history • If abuse suspected, client should be interviewed alone for at least part of the time • Others may be interviewed separately • Include general questions about feelings of safety • If offered, note nature, frequency and severity of abusive events • “Do you have family or friends who are willing to nurture, listen, and assist you?” • (More practicable) “Do you feel safe at home?”
Interview with family members • Avoid confrontation • Explore if caregiving responsibilities are burdensome • Acknowledge the caregiver’s difficult role • Are there any recent stressful events? • Interview patient, family member separately
Situations suggesting elder abuse (1) • When there is a delay between the injury or illness and the seeking of medical attention • When the accounts of the patient and the caregiver do not agree • When the severity of the injury does not fit the explanation given by the caregiver • When the explanation of the patient or caregiver is implausible or vague • When visits to the emergency department for chronic disease are frequent despite appropriate care and adequate resources
Situations suggesting elder abuse (2) • When a functionally impaired patient presents for care without a designated caregiver in attendance • When laboratory findings are inconsistent with the history • When the caregiver is reluctant to accept home health care or to leave the elderly person alone with a health care practitioner
Signs of elder abuse (1) • Behavior—withdrawal by the patient infantilization of the patient by caregiver; caregiver insists on giving history • General appearance—poor hygiene, inappropriate dress • Skin/mucous membranes—signs of dehydration, multiple skin lesions, bruises, pressure ulcers, deficient care for skin problems • Head and neck—traumatic alopecia
Signs of elder abuse (2) • Trunk—bruises, welts (shapes may suggest implement) • Genitourinary area—rectal bleeding, vaginal bleeding, pressure sores, infestations • Extremities—wrist or ankle lesions suggesting restraints or immersion to burn • Musculoskeletal—occult fracture, pain, gait disturbances • Mental and emotional health—depression, anxiety
Roles of nursing and social work • Members of interdisciplinary team • May be appointed as coordinator to ensure pertinent data are recorded correctly • Relevant parties are contacted and informed • Necessary care is available 24 hours per day • Inservice education on elder abuse
Reporting elder abuse • Reporting of suspected or confirmed abuse is mandatory in all states if abuse occurs in an institution • Mandatory in most states if it occurs at home • Adult protective services • Burden of proof does not rest on the reporter • Reporting suspected abuse without claim of abuse • May be anonymous
Formal evaluation • What is your nursing diagnosis for S. T.? • What is your desired outcome? • What steps will you take? • What are your appropriate interventions?