Download
1 / 65
750 likes | 1.4k Views
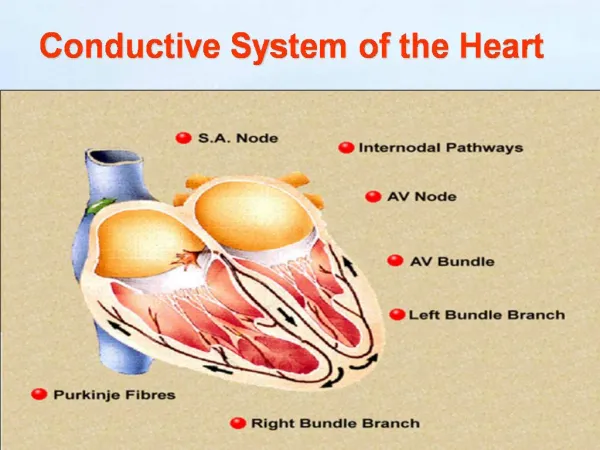
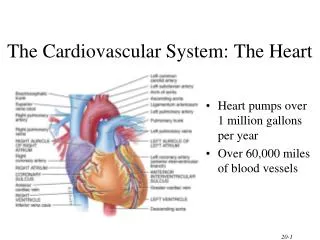
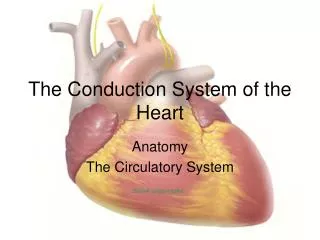
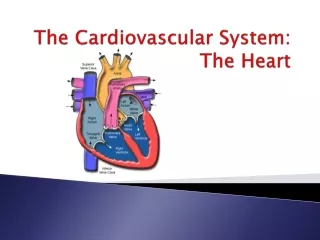
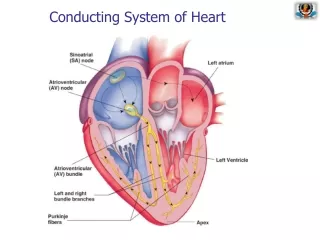
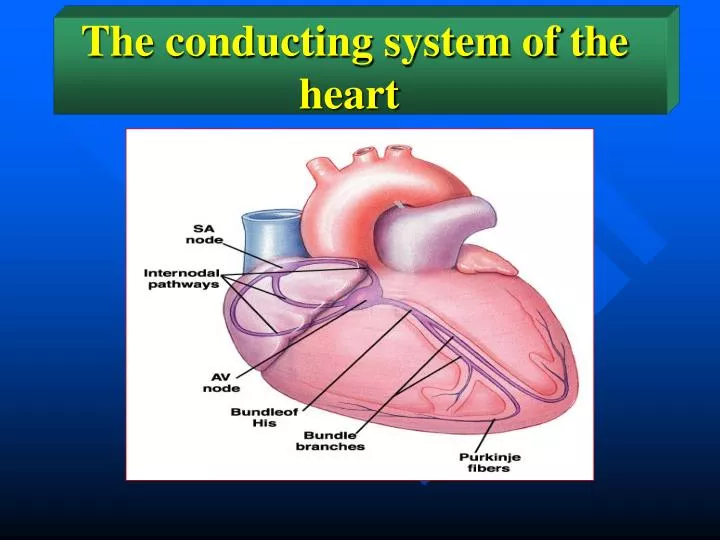
The conducting system of the heart. The conducting system of the heart. 1. The nodal system: Which consists of two nodes in the right atrium: The sinoatrial node (also called the S-A node or the sinus node). The atrioventricular node (also called the A-V node).

E N D
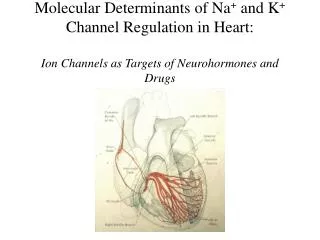
The conducting system of the heart 1. The nodal system: Which consists of two nodes in the right atrium: The sinoatrial node (also called the S-A node or the sinus node). The atrioventricular node (also called the A-V node). 2. The internodal pathway: 3. The purkinje system (also called the His-Purkinje system): The atrioventricular bundle (also called the A-V bundle or the bundle of His). The right and left bundle branches. The Purkinje fibers.
Functional histology 1. The contractile muscle fibers: Differences between the contractile cardiac muscle fibers and skeletal muscle fibers. 2. Nodal fibers of the S-A and A-V nodes: 3.The Purkinje fibers of the Purkinje system:
STRUCTURE OF A MYOCARDIAL CELL Mitochondria Sarcolemma T-tubule SR Fibrils
Myocardial Contraction Myocardial fiber Myofibril myosin Myofilaments actin relaxed contracted
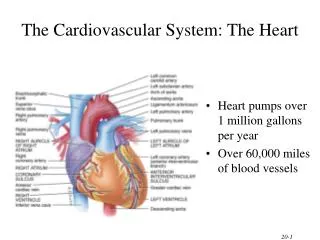
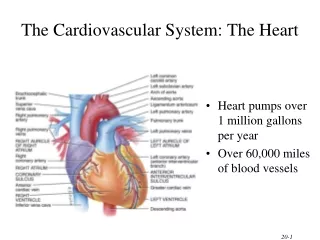
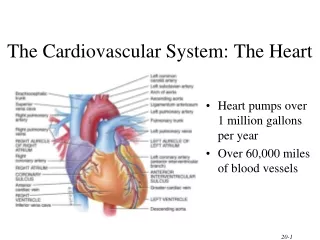
1. The main function of the atria is to accommodate blood returning to the heart during ventricular systole until it is passed on to the ventricles during ventricular diastole. 2. The pumping action of the atria increases the ventricular filling. This increases the pumping capacity of the ventricles by 15-20%. Functions of the atria
The ventricles are the central pumps of the circulatory system. They pump the venous return which they received by the atria. The right ventricle pumps the systemic venous return into the pulmonary circulation and the left ventricle pumps the pulmonary venous return back into the systemic circulation. Function of the ventricles
Ventricular volumes End-diastolic volume (EDV): is the volume of blood in the ventricle at the end of diastole. It is about 130 ml. End-systolic volume (ESV): is the volume of blood in the ventricle at the end of systole. It is about 55 ml. Stroke volume (SV): is the volume of blood that is pumped by the ventricle per beat. It is equal to the difference between the EDV and ESV. Its is about 75 ml. Diastolic filling volume (DFV): is the volume of blood which flows from the atrium into a ventricle during diastole. It is equal to the difference between the EDV and the ESV. It is about 75 ml.
Properties of the cardiac muscle The heart has four basic properties which are essential for its functioning as the central pump of the CVS. These are: 1. Autorhythmicity 2. Conductivity 3. Excitability 4. Contractility
Autorhythmicity Automaticity Rhythmicity Autorhythmicity Autorhythmicity is a myogenic innate property of the heart independent of its nerve supply.
Autorhythmicity The conducting system of the heart is responsible for generating rhythmic, electrical impulses which drive the heart to beat in a rhythmic way. The focus which generates the highest frequency of impulses is he one that drives the whole heart and is called the pacemaker of the heart. The normal pacemaker of the human heart is the S-A node.
Autorhythmicity There are several possible sites in the conducting system that can act as possible pacemakers: Sino-atrial (SA) node Atrio-ventricular (AV) node Purkinje system If the primary pacemaker is damaged or blocked, the secondary pacemaker takes over. If the flow of impulses from the atria to the ventricles stops completely, the tertiary pacemaker takes over and the ventricles continue to beat at the idioventricular rhythm.
THE RESTING MEMBRANE POTENTIAL OF THE CARDIAC CELL • IN OUT K+ • K+ 5mEq 145mEq • Na+ • Na+ 145mEq 10mEq Em= -60LogKi/Ko -90mv
The pacemaker potential The pacemaker cells are characterized by having an unstable membrane potential. This is the basis for automaticity
AUTOMATICITY Na+ K+ Gradually increasing PNa K+ Na+ -0 -60 mV THRESHOLD RESTING
The pacemaker potential The pacemaker cells are characterized by having an unstable membrane potential. After firing an action potential, the membrane potential decreases i.e. the membrane depolarizes gradually from a basal value of ~ -60mV to a critical firing level of –45 mV. At this level, an action potential is fired and the cycle is repeated. The gradual depolarization of the S-A nodal cells is called the pacemaker potential or the prepotential. The early part of the pacemaker potential is caused by a decrease in the permeability of the membrane to K+. The late part is caused by Ca++ influx through the transient (T-type) Ca++-channels.
The pacemaker action potential When the pacemaker potential reaches the critical level (~ -45 mV), an action potential is produced in the pacemaker cells. This action potential propagates to the surrounding myocardial cells.
ELECTROPHYSIOLOGY OF THE CONTRACTILE FIBER AMP +20 1 To oscilloscope 2 0 3 0 mv Cardiac Cell 4 -90 0 300 t (msec)
PHASE 0 = Rapid Depolarization (inward Na+ current) 1 1 2 0 2 = Plateau (inward Ca++ current) 3 = Repolarization (outward K+ current) 0 MEMBRANE POTENTIAL (mV) 4 = Resting Potential 3 4 -90 TIME
0 0 mv mv -90mv -90mv 0 mv -60mv ACTION POTENTIALS FROM DIFFERENT AREAS OF THE HEART ATRIUM VENTRICLE SA NODE time
ACTION POTENTIALS VENTRICULULAR CELL SAN 1 2 0 0 0 3 0 3 4 -50 -50 MEMBRANE POTENTIAL (mV) 4 -100 -100
The pacemaker action potential differs from the action potential of the contractile myocardial cells in the following: Depolarization phase is mainly due to Ca2+ influx through long-lasting (L-type) Ca2+-channels. Depolarization phase is relatively slow to develop. There is no plateau phase. Repolarization immediately follows depolarization.
Ectopic foci An ectopic focus is an area in the contractile myocardium, which discharges electrical impulses. Normally, the contractile myocardium has a stable resting membrane potential and is incapable of discharging impulses. Under some non-physiological conditions, some myocardial cells acquire rhythmic electrical activity and act as foci that send un-timed electrical impulses or might even take over the heart and act as the pacemaker.
Chronotropism Chronotropism means an influence on the heart rate. A +ve chronotropic factor (or effect) is one that increases the heart rate. A –ve chronotropic factor (or effect) is one that decreases the heart rate.
Factors that influence cardiac autorhythmicity Several factors influence autorhythmicity by influencing the rate of discharge from the heart pacemaker. These factors could be classified into: Nervous factors Chemical factors Physical factors Mechanical factors
Nervous factors The most important factor in the regulation of the heart rate is the activity of the cardiovascular centers in the medulla oblongata. This activity is transmitted to the heart via its sympathetic and parasympathetic nerve supply.
Sympathetic nerve supply There is a resting sympathetic tone that tends to increase the heart rate up to 120 beats/min. This tone is weak and is masked by the strong inhibitory vagal tone that decreases the heart rate down to 75 beats/min during rest. However, stimulation of the sympathetic cardiac nerves has a +ve chronotropic effect. The heart rate may g up to 200 beats/min. The sympathetic chemical transmitter noradrenaline decreases the permeability of the pacemaker membrane to K+. This accelerates the depolarization of the membrane → shortens the duration of the pacemaker potential → increases the frequency of discharge of impulses from the S-A node → increases the heart rate.
Parasympathetic nerve supply There is a resting inhibitory vagal tone that keeps the heart rate at its resting level of ~ 75 beats/min. During deep quite sleep, the vagal tone increase and the heart rate decreases down to 60 beats/min. Vagal stimulation has a –ve chronotropic effect. The parasympathetic chemical transmitter acetyl choline increases the permeability of the pacemaker membrane to K+. This slows down the depolarization of the membrane → prolongss the duration of the pacemaker potential → deccreases the frequency of discharge of impulses from the S-A node → decreases the heart rate.
Cutting or blocking the vagal nerve supply to the heart (e.g., by atropine) leads to an increase in the heart rate up to ~ 120 beats/minute. This is the sinus rhythm boosted by the resting sympathetic tone. If this is followed by cutting or blocking the sympathetic nerve supply to the heart (e.g., by atenolol), the heart rate decreases down to 105 beats/minute; the natural inherent sinus rhythm. Cutting or blocking the sympathetic nerve supply to the heart with an intact vagal parasympathetic supply produces no significant change in heart rate, i.e. it remains at its resting level of ~ 75 beats/minute.
Chemical factors Adrenaline and noradrenaline are released into the blood under conditions of stress. Both substances have a +ve chronotropic effect.
Physical factors Arise in body temperature by 1 °C increases the heat rate by 20 beats/minute. The rise in body temperature increase the heart rate by increasing the permeability of he membrane to Ca++ during the pacemaker potential and increasing the speed of ionic fluxes across the membrane during the action potential. The only physiological condition that rises body temperature above the normal resting range is muscular exercise.
The sick sinus syndrome This is a pathological condition where there is bradycardia accompanied by frequent attacks of dizziness and syncope. It is caused by a disease of the S-A node depressing its activity and decreasing the rate of impulse generation. This condition is treated by implantation of an artificial pacemaker.
Conductivity Impulses can spread easily between cardiac muscle fibers. Yet, conduction in the heart is normally carried out by the specialized conducting system to ensure the spread of the excitation wave from the S-A node to all over the heart in certain pattern.
The origin and pathway of the cardiac impulse The normal cardiac impulse originates inside the S-A node, the normal pacemaker of the heart. The impulse is then conducted to the surrounding atrial wall through the peripheral S-A nodal tissue. Then it propagates in three pathways: To the right atrium through the atrial muscle fibers To the left atrium through the interatrial ‘Bachmann’s bundle’ To the A-V node through the internodal bundles
The impulse picked up by the A-V node is delayed for 0.1 – 0.15 second, then passed on to the A-V bundle. The A-V bundle conducts the impulses to the buddle branches. Then from the bundle branches to the Purkinje fibers on to the ventricular muscle fibers.
Important functional characteristics of the A-V node The A-V node is characterized by: Very slow conductivity:This delays the transmission of impulses to the ventricles (A-V nodal delay). This delay allows the atria to finish with their systole before passing the impulse to the ventricles to start ventricular systole. Long absolute refractory period after conducting an impulse:This limits the number of impulses that can be transmitted from the atria to the ventricles to 230 impulse/min. This protects the ventricles from receiving high frequency of impulses from the atria.
Factors that influence conductivity Sympathetic stimulation accelerates conduction and decreases the A-V nodal delay. Parasympathetic stimulation slows conduction and may produce various degrees of heart block.
The one-way conduction in the A-V bundle The A-V bundle conducts impulses only in one direction, i.e. from the A-V node to the bundle branches. This prevents the reentry of impulses from the ventricles into the atria.
Excitability Excitability is the ability to respond to stimuli. The resting membrane potential of the contractile fibers is stable at about – 90 mV. When an effective stimulus is applied, a propagated action potential is produced in the cell membrane.
PHASE 0 = Rapid Depolarization (inward Na+ current) 1 1 2 0 2 = Plateau (inward Ca++ current) 3 = Repolarization (outward K+ current) 0 MEMBRANE POTENTIAL (mV) 4 = Resting Potential 3 4 -90 TIME
Phase 0 (Rapid depolarization): It is caused by the rapid influx of Na+ into the cell. Phase 1 (Early partial repolarization): During this phase, the permeability of the membrane to Na+ is rapidly reduced, but the membrane permeability for both Ca2+ and K+ increases. The overall effect is a small change in the membrane potential toward the resting membrane potential (repolarization). Phase 2 (Plateau of the action potential): This coincides with an increased permeability for Ca2+. The inward movement of Ca2+ and the decreased efflux of K+ maintain the membrane potential near zero during this phase of the action potential. Phase 3 (Rapid repolarization): due to a reduction of the inward Na+ and Ca2+ currents and a large increase in the outward K+ current. Phase 4 (Complete repolarization): the membrane goes back to the resting level (- 90 mV). Na+-K+ pump works to drive the excess Na+ out and the excess K+ in.