Download
1 / 36
360 likes | 532 Views
1. Emergency Contraception for Non-Clinical Providers in Washington State. 2. Learning Objectives. Understand the critical role of emergency contraception (EC) in pregnancy prevention Understand EC safety and effectiveness Clarify role of non-clinical providers in educating clients about EC

E N D
1 Emergency Contraceptionfor Non-Clinical Providersin Washington State
2 Learning Objectives • Understand the critical role of emergency contraception (EC) in pregnancy prevention • Understand EC safety and effectiveness • Clarify role of non-clinical providers in educating clients about EC • Identify mechanisms for raising awareness of EC within client population • Increase awareness of EC resources
3 Why Is Emergency Contraception Needed? • Around 10 million couples have sexual intercourse every night in America • Approximately 27,000 condoms break or slip • Even perfect contraceptors can and do experience contraceptive failure Source:Trussell & Kowal, 1998.
4 Current Proportion of Unintended Pregnancy United States: 49% Washington State: 55% Source:Henshaw, 1998; Schrager, 1997.
5 Definition of Unintended Pregnancy • Pregnancy that is unwanted or mistimed at conception • Does not mean unwanted births/unloved children • Does mean less opportunity to prepare: • Pre-pregnancy risk identification • Management of preexisting conditions • Changes in diet and vitamins • Avoidance of alcohol, toxic exposure, and smoking
6 Consequences of Unintended Pregnancy • Approximately half of all unintended pregnancies end in abortion • Greater risks for mother • depression; physical abuse; not achieving educational, financial, career goals; relationship challenges • Greater risks for child • low birthweight, dying in first year of life, abuse, and neglect Source:Institute of Medicine, 1995.
7 The Institute of Medicine Recommends That the Nation Adopt a New Social Norm All pregnancies should be intended–that is, they should be consciously and clearly desired at the time of conception. Source:Institute of Medicine, 1995.
8 Emergency contraceptionprevents pregnancyAFTER sex
9 Emergency ContraceptionObstacles to Use • Most women don’t know about the method • 11% of women know the basic facts about EC • 1% have used it • Most health care providers do not routinely discuss EC with their clients • approximately 1 in 10 routinely discuss EC • These data are supported by PATH’s local assessment Source: Kaiser Family Foundation, 1997.
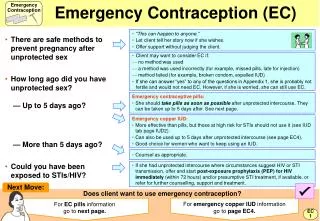
10 What Is Emergency Contraception? • Emergency Contraceptive Pills (ECPs) • Have been in use since the 1960s • Often referred to as “the morning-after pill” • Birth control pill hormones taken in high doses within 3 days (72 hours) of unprotected sex • IUD Insertion • Within 5 days (120 hours) of unprotected sex • Can also be a long-term contraceptive method
ECPs Can Be Used Any Time Unprotected Intercourse Has Occurred 11 • A woman was raped • No contraception used • Condom slipped, leaked, or broke • Diaphragm or cervical cap inserted incorrectly, removed too soon, or torn • Two consecutive birth control pills were missed • An IUD was partially or totally expelled • A three-month contraceptive injection was missed by more than two weeks • A one-month contraceptive injection was missed by more than three days
12 Limitations of ECPs • ECPs are not as effective as regular contraceptive methods • Should be used as a bridge to long-term birth control options • ECPs do not protect against STDs
13 Are ECPs Safe? • ECPs are safe and easy to use • The amount of active ingredient (hormone) is small • Short-term use • Hormones leave the body quickly Source: WHO, 1996.
14 What if a Woman Is Already Pregnant? • ECPs cannot dislodge an established pregnancy • They do not cause abortion • ECPs do not affect fetal development Source: FDA, 1997.
Progestin-only Reduces the risk of pregnancy by 89% Side effects Nausea (23%) Vomiting (6%) Estrogen and Progestin Reduces the risk of pregnancy by 75% Side effects Nausea (50%) Vomiting (20%) 15 Two Types of ECPs Both Methods: First dose within 72 hours after intercourse Second dose 12 hours later Source: Task Force on Postovulatory Methods of Fertility Regulation, 1998.
16 Effectiveness: Single-Use Progestin Only 100 women have unprotected sex in the 2nd or 3rd week of their cycle 8 will become pregnant without emergency contraception 1 will become pregnant using progestin-only ECPs (89% reduction) Adapted from ARHP, 1999. Source: Task Force on Postovulatory Methods of Fertility Regulation, 1998.
17 Effectiveness: Single-Use Combination Pill 100 women have unprotected sex in the 2nd or 3rd week of their cycle 8 will become pregnant without emergency contraception 2 will become pregnant using combined ECPs (75% reduction) Adapted from ARHP, 1999. Source: Trussell, Rodriguez, and Ellertson, 1998.
18 How Do ECPs Work? • The same way as ordinary birth control pills by • Preventing or delaying the release of a woman’s egg (ovulation) • ECPs may affect the uterine lining so that a fertilized egg cannot implant • ECPs may prevent fertilization by affecting the movement of the sperm and their ability to fertilize an egg • Timing impacts how ECPs work Source: Swahn et al., 1996; Ling et al., 1979; Rowlands et al., 1986; Ling et al., 1983; Kubba et al., 1986; Taskin et al., 1994; Von Hertzen & Van Look, 1996.
19 Medical Definition of Pregnancy • NIH, FDA, and ACOG all define pregnancy as beginning with implantation • It takes about 6 days for a fertilized egg to begin to implant • Intervention within 72 hours cannot result in abortion • ECPs are not effective if a women is already pregnant Source: Code of Federal Regulations, 1998; Hughes, 1972.
20 Providing EC Information • Some women will want to base their decision on whether to use ECPs on how they work. • It is important that women clearly understand how pills are believed to work so they can make an informed choice.
21 Key Points on Mechanism of Action • ECPs will not interrupt or harm an established pregnancy • ECPs will not affect future fertility • ECPs are not the same as the “abortion pill” (RU486), which is used after pregnancy is already established • ECPs work through various mechanisms
22 What are the key messages to get across to your clients?
23 Key Messages for Clients • 72-hour time frame (but sooner is better) • Safe and effective • Mechanism of action (informed choice) • Do not cause abortion • Side effects: nausea and vomiting • Not as effective as other contraceptives for regular use • Potential bridge to regular contraception • ECPs do not protect against STDs • Sources for accessing ECPs
24 What other issues might be of importance to clients?
25 Key Topics of Importance to Clients • No future impact on childbearing • No threat to potential pregnancy • Not abortion • Religion (individual’s religious background not always predictive of EC interest) • Expense of ECPs (covered by Medicaid) • Confidentiality • Adolescents • Diverse communities • Interpreters
26 Where Can Women Get ECPs? • Advance-of-need prescribing/distribution • Doctor or clinic • Walk-in visit/appointment • Telephone screening • Some pharmacies in Washington State can provide ECPs directly to women
27 Advance Distribution or Advance-of-Need Prescribing of ECPs • ECPs are more effective when taken sooner • Advance prescription reduces access barrier • Women are not more likely to use ECPs repeatedly • Advance prescription does not decrease the use of other birth control methods Source: Glasier and Baird, 1998.
28 Expanded Access Through Pharmacies in Washington State • Collaborative drug therapy agreement between pharmacist and independent prescriber • Trained pharmacists participating in a collaborative agreement can provide ECPs directly to women who request them • Currently over 145 pharmacies participating • In first 16 months of project pharmacists wrote and filled almost 12,000 prescriptions for ECPs
29 Medicaid Coverage of ECPs • Medicaid covers ECP prescriptions • Medicaid covers pharmacist counseling time for women who receive ECPs directly from pharmacist • Medicaid will also cover advance-of-need prescriptions
30 Cost of ECP • For prescriptions written by medical providers (MDs, ARNPs, PAs): • If covered by insurance: $5-10 co-pay • If no insurance coverage: • Plan B™: $18-35 • Preven™: $20-35 • Note: client also must pay for office visit to get prescription • For prescription and consultation at pharmacy: • Pills and counseling: $35-45 • As dedicated products become more widely used, cost may rise slightly: $40-45
31 Resources Included in Provider Packet • Q & A for non-clinical providers • Key messages to convey to clients • EC referral card • Emergency Contraception: Client Materials for Diverse Audiences booklet • List of pharmacies that provide ECPs in Washington State • EC reference list
Provides EC information in 13 languages: Amharic Arabic Cambodian Chinese English Haitian-Creole Korean Laotian Portuguese Russian Somali Spanish Vietnamese 32 EC Materials for Diverse Audiences
33 Clinics and Pharmacies That Provide ECPs in Your Area • EC Hotline • 1-888-NOT-2-LATE (1-888-668-2528) • EC website • http://not-2-late.com • Planned Parenthood website • http://plannedparenthood.org • Washington State Family Planning Hotline • 1-800-770-4334
34 How will you emphasize ECPs in your setting?
35 Tell Your Clients About ECPs by: • Routinely discussing ECPs • Making ECP materials available in agency setting • Encouraging advance-of need-prescribing