Download
1 / 33
330 likes | 445 Views
MOCK EXAM!!. End of block assessment. Cummulative Grade Log Book Consultant Assess. Portfolio(3) SAQ GRADE MCQ GRADE 14 Short answer Questions X10 Marks= 140 30 MCQ X10 Marks= 300 Marks. SAQ Under 45 % - U 45 - 49 B 50 - 75 S Over 75 – E MCQ

E N D
End of block assessment Cummulative Grade • Log Book • Consultant Assess. • Portfolio(3) • SAQ GRADE • MCQ GRADE • 14 Short answer Questions X10 Marks= 140 • 30 MCQ X10 Marks= 300 Marks • SAQ Under 45 % - U 45 - 49 B 50 - 75 S Over 75 – E • MCQ Under 50 - U 50 - 59 B 60 - 80 S Over 80 - E
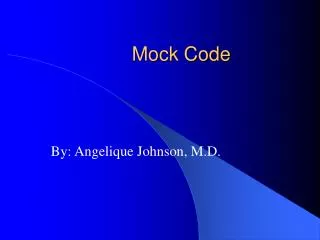
1. • g) Face presentation • Submento-bregmatic • h) Deflexed OP • Occipito-frontal • i) Brow presentation • Occipito-mental • j) Normal vertex • Sub-occipitobregmatic • Name the parts of fetal skull as indicated. • Occipital bone • Posterior fontanelle • Sagittal suture • Frontal bone • Anterior fontanelle • Parietal bone • 2. Name the presenting diameter in various • presentation
2. Mrs Turvey is a 28 year old woman and attends the ANC at 36 weeks gestation in her first pregnancy with a breech presentation What is the definition of presentation in obstetric practice The part of the fetus that is at the pelvic inlet/lower pole of the uterus b) List three possible reasons for the clinical situation Prematurity, multiple pregnancy, polyhydramnios, placenta praevia, uterine abnormality. c) List 2 management options. C/S; ECV d) Name 3 contraindications to ECV. Multiple pregnancy, Antepartum haemorrhage, placenta praevia e) List one fetal complication of breech presentation Birth trauma- head entrapment, fractures; cord prolapse; fetal distress; PPH
3. A 30yr old woman attends for contraceptive advice. She is epileptic and is on phenytoin to control her fits. Her BMI is 35.She has a new partner and she does not wish to get pregnant. Her ex-husband had a vasectomy so there were no contraceptive issues List three issues that will influence your choice of contraception. Epileptic , High BMI, New relationship b)List 3 suitable methods Mirena POP Implant /Depoprovera Condom (protect from STI) c)List 2 contraceptive choices that would not be optimum for this lady & why? COC- enzyme inducer, Raised BMI Sterilisation- as recently divorced and has a new partner
4. Mrs C is a 36 yrs old in her 1st pregnancy. She was admitted at 39 wks with SROM. Contraction failed to start and labour was induced with prostaglandin 2 days later. She progressed to 5 cm dilatation.. CTG shows baseline of 170bpm with variability of 2 beats. There are broad variable decelerations. A FBS was performed( pH= 7.19,base excess=-10.5) a) What does CTG stand for? Cardiotocograph b) What is the normal range of fetal baseline heart rate? 110-160 bpm c) What is the definition of deceleration? Downward deflection of baseline >15 beats for>15 sec. d) List one possible reason in this patient to explain the CTG feature. Infection e)List 2 circumstances in labour where FBS is inappropriate (1)Maternal infection – HIV, Hepatitis ( 2) Bleeding disorders in fetus (thrombocytopenia), haemophilia f) What is your interpretation of pH & what is your management plan? Acidosis, C/S
5. Syntometrine is used commonly on labour ward. Why is this drug used? To prevent or treat PPH b) When is it administered? With the delivery of anterior shoulder c) Give 2 routes of administration? IM,IV d)List 2 side effects. Nausea, vomiting HTN e) List 3 contraindication to its use. HTN, Cardiac disease, undelivered twin f) Give an alternative drug that can be prescribed. Syntocinon
6. A 45 yr has been diagnosed with Stage 1b Ca Cx. She is admitted to undergo an operation. What is stage 1b Ca Cervix? Clinically visible lesion limited to the cervix. b) What is the most likely op she is admitted for? Radical hysterectomy +pelvic node clearance(Wertheim’s hysterectomy) c) List 4 short term complications. Anaesthetic complication, Haemorrhage, bowel/ureteric injury, Peritonitis, Ileus, UTI, thromboembolism d) List 4 long term complications. Sexual dysfunction Vesico-vaginal fistula Lymphoedma Pain Depression
7. You are called to see a 25 yr old who is 3 days postnatal and has developed chest pain. She complains of lower left sided pain. She is slightly breathless. Her BP= 150/89, pulse= 98/min. She had uncomplicated forceps delivery. What is the most probable diagnosis? PE b) What important blood investigation would you perform? ABG c) What 2 features you would expect this test to show if your diagnosis was correct? Pco2-N, po2-low d) List 3 other investigation you will perform & why? CXR(R/O chest infection); ECG- tachycardia, S1Q3T3; V/Q scan or CTPA (to confirm the diagnosis) e) How should she be treated? LMWHs/c, Warfarin(PO) f) List 2 pre-pregnancy risk factors. Thrombophillias, Obesity, family History
8. A 25 yr old G5P4 is admitted at 38 weeks gestation with sudden onset of painless vaginal bleeding. She lost 400ml blood. Her P88/min BP= 105/65. On abd. exam- abdomen is soft ,non tender. The fetus is lying transversely and fetal trace is normal with a baseline of 140bpm. What is most likely diagnosis? Placenta Previa b) Give 4 reasons to support the diagnosis. Painless bleeding; Soft abdomen; No fetal compromise & Transverse lie at term c) List 2 other differential diagnosis? Placental abruption; local cause of bleeding d) What is your immediate management? IV access, bloods-FBC, cross match 4 U, coagulation screen Fetal monitoring (CTG) Monitor maternal wellbeing e) What investigation will confirm diagnosis? USS for placental localisation
9. 70 yr old attends with H/O urinary incontinence, in particular frequency, urgency with incontinence. What is your diagnosis Detrusor overactivity/ overactive bladder syndrome b) What will be the features on urodynamic trace? Detrusor contraction provoked by bladder filling. c) What is the maximum bladder capacity on a UDS trace? Maximum volume after which she is incontinent d) List 2 non-surgical (conservative) management. Bladder training ; Drugs; Fluid advice e) Name 2 drug treatments. Anticholinergics: Oxybutynin Antimuscarinic: Tolterodine, trospium & solifenacin Antidepressant:Imipramine f) List 2 other types of incontinence Stress Incontinence Retention with overflow, Neurogenic
10. An 18yr old woman presents to gynae admission with history of abdominal pain of 4 hours duration and PV bleeding, seven weeks of amenorrhea and a positive pregnancy test. What are your likely diagnosis? Ectopic pregnancy; Threatened miscarriage b) List 5 investigations. FBC, G&S, βhCG, S.progesterone, pelvic USS, diagnostic lap c) What treatment options are available for your diagnosis? Ectopic – Salpingectomy, Methotrexate Threatened miscarriage – expectant, ERPC if incomplete miscarriage
11. A 32 yr old presents to ANC at 35weeks in her 1st pregnancy. She has been low risk . Her SFH = 30cm and fetus is lying longitudinally, cephalic presentation. The fetal heart can be heard. What is your diagnosis? IUGR b) What one investigation will be most useful? USS c) List 3 fetal causes of the condition. Placental insufficiency, constitutional, chromosome, infection d) From your investigation which 3 factors are helpful? Biometry; liquor volume; umbilical artery doppler e) List 1 neonatal complication. Hypothermia, fits, Jaundice f) List 1 long term complication HTN
12. Mrs Blood is 43 yr old suffering with heavy painful but regular periods. This has gradually worsened over the last 2 years. List 3 investigations you may wish to do. FBC Endometrial sample/hysteroscopy USS b) List 4 medical options. Mefenamic acid Tranexamic acid COC, Danazol Mirena IUS c) If she has completed her family ,what are her surgical option? Endometrial ablation - balloon, MEA, Novasure Endometrial resection - TCRE Hysterectomy
13.Andrew Blank is 28 Yr old car mechanic who smokes 20/day and enjoys a night out in the pub over the weekend. His partner and he has been trying for a baby for 5 years and attend for investigation. The results of semen analysis are: Volume- 2ml, Count- 10 million/ml, motility-20% motile, morphology- 90% abnormal forms List 1 normal finding. Volume b) List 2 abnormal findings Poor count, poor motility, abnormal morphology. c) Give 2 aetiological factors that could cause this result. Infection, trauma/surgery d) List 2 advice you give to this patient. Stop smoking, reduce alcohol, loose underwear & dietary advice e)What treatment options are available? ICSI, IVF, donor insemination or adoption
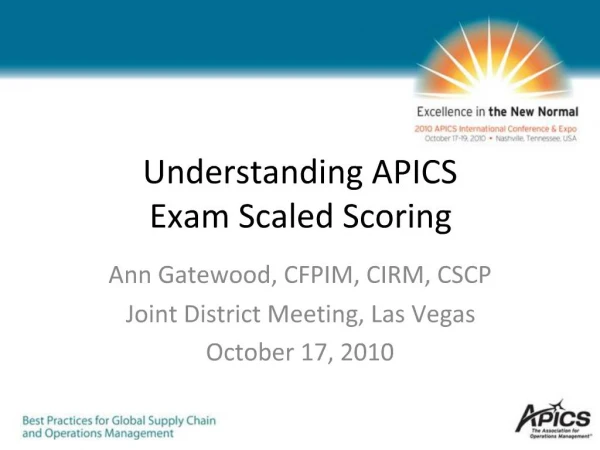
14. Look at the image and answer the questions. What is the diagnosis? Vulval candidiasis b) Name the organism. Candida Albican c) What 2 symptoms this patient may have? Itching; vaginal discharge. d) How would you treat it? Clotrimazole 500mg PV e) What investigation would you do to confirm diagnosis? HVS-microscopy f) List 3 predisposing condition Pregnancy, diabetes, antibiotic use, immuno suppressed patient
MCQ 1. The following statements about contraception are correct: a) The combined oestrogen/progestogen contraceptive pill usually increases menstrual blood loss b) Inflammatory bowel disease is a recognised contraindication to the combined oestrogen/progestogen pill c) The progestogen-only contraceptive pill is recognised to cause intermenstrual bleeding d) The intrauterine contraceptive device is associated with a higher risk of pelvic inflammatory disease than oral contraception e) Laparoscopic sterilisation of the female by Falope rings can be successfully reversed in over 90% of cases FFTTF
2. Intrauterine contraceptive devices: a) Should not be inserted at the time of suction termination of pregnancy b) Are radio-opaque c) Should be removed in early pregnancy if the threads are visible d) Should preferably be inserted mid cycle e) Are contraindicated in patients with rheumatic heart disease FTFFT 3. Ectopic pregnancy: a) Is most commonly found in the fallopian tube b) Is associated with daily doubling of serum beta-hCG levels c) Is associated with a past history of pelvic infection d) Is a recognised complication of in vitro fertilisation and embryo transfer e) Is best diagnosed by pelvic examination under anaesthesia TFTTF
4. The following serum levels are compatible with the condition named: a) High androstenedione and polycystic ovarian syndrome b) High sex hormone binding globulin and polycystic ovarian syndrome c) High prolactin and anovulation d) Low oestrogen and endometrial hyperplasia e) Low follicular stimulating hormone and menopause 5. The following statements about Testosterone are correct: a) Levels in excess of 5 nmol/L should raise the possibility of an ovarian tumour b) Must always be elevated in Polycystic ovarian syndrome c) Results from peripheral conversion of oestrogen d) Is reduced in testicular feminisation syndrome e) If given to men will improve their sperm counts TFTFF TFTFF
6. Fibromyomata (Leiomyomas) a) Are composed of striated muscle b) Can cause heavy menses c) Have over a 20% potential to form a sarcoma d) Can occur in the uterine cervix e) Atrophy during pregnancy 7. The following is a recognized treatment of urinary stress incontinence: a) Vaginal hysterectomy b) Insertion of a ring pessary c) Posterior colpoperrineoraphy d) Colposuspension e) Amitriptyline FTFTF FFFTF
8. The following are used in the treatment of anovulatory infertility: a) Tamoxifen b) Norethisterone c) Danazol d) Human chorionic gonadotrophin e) Dianette 9. Hormone replacement therapy protects postmenopausal women against: a) Osteomalacia b) Coronary artery thrombosis c) Deep venous thrombosis d) Atrophic vaginitis e) Cerebral haemorrhage FFFFF FFFTF
10. The following characteristically cause heavy regular menses: a) Endometrial carcinoma b) Adenomyosis c) Cervical carcinoma d) Endometriosis e) Granulosa cell tumour of the ovary 11. The following drugs may be used for the treatment of menorrhagia: a) Clomiphene b) Mefanamic acid c) Danazol d) Tranexamic Acid e) Combined oestrogen-progestogen oral contraceptives FTFFF FTTTT
12. The following are useful in the treatment of dysfunctional uterine bleeding in a 45 year old woman: a) Dilatation and curettage b) MIRENA c) Myomectomy d) Depo-Provera e) Hysteroscopy FTFFF 13. The following statements relating to cervical intra-epithelial neoplasia (CIN) are correct: a) Screening for CIN should start at the age of 22 years b) It is associated with a history of multiple sexual partners c) It arises in the squamo-columnar junction of the cervix d) Diathermy large loop excision of the transformation zone (LLETZ) is the treatment of choice for persistent CIN I e) Hysterectomy is the first line treatment for CIN III FTTTF
14. Endometrial cancer: a) Is the commonest cause of postmenopausal bleeding b) Is more common in multipara than in nullipara c) It’s risk factors include diabetes mellitus d) Is a recognized complication of combined hormone replacement therapy e) Stage 1 lesions are usually treated with radical hysterectomy 15. Termination of pregnancy: a) May legally be performed at any gestation when there are severe fetal abnormalities b) Can be performed using prostaglandins c) Must be approved by three independent medical practitioners d) May be carried out using Mifepristone (RU 486) e) Is safely carried out by suction evacuation in the second trimester FFTFF TTFTF
16. Asymptomatic bacteriuria a) occurs in more than 15 per cent of pregnant women b) converts to overt infection in 5% of untreated patients c) is associated with preterm labour d) causes leucocytosis e) causes epithelial cells to be present in urine 17. The following investigations are performed routinely at the first antenatal visit: a) Haemoglobin concentration b) Blood group and atypical antibodies c) Human chorionic gonadotrophin d) Serum alpha-fetoprotein e) Midstream urine culture FFTFF TTFFT
18. The following statement(s) about fetal physiology is/are correct: a) The normal fetal heart rate varies between 70 and 110 beats per minutes b) The amniotic fluid is formed mainly from fetal urine in late gestation c) The umbilical vein carries deoxygenated blood d) Fetal breathing movements increase during parturition e) Umbilical artery Doppler velocimetry characteristically shows a resistance pattern FTFFT 19. The following statements about amniocentesis are correct: a) It is best performed under ultrasound guidance b) It can cause miscarriage c) It can cause Rhesus iso-immunization d) The maternal serum alpha-fetoprotein, oestriol and bHCG(Triple test) is as accurate as amniocentesis in the diagnosis of Down’s syndrome e) High levels of amniotic fluid alpha-fetoprotein may be associated with fetal neural tube defects TTTFT
20. Concerning diagnostic ultrasound in pregnancy: a) Crown-rump length measurement can be used to estimate gestational age after 32 weeks gestation b) Fetal abdominal circumference is a better index than bi-parietal diameter in the diagnosis of intrauterine growth restriction c) It is recognised to diagnose neural tube defects d) It is recognised to diagnose Down’s syndrome e) The fetal biophysical profile includes umbilical artery Doppler flow velocimetry 21. Lactation is associated with: a) Reduced fertility b) Release of oxytocin c) High prolactin levels d) Uterine contractions e) Superficial dyspareunia FTTFF TTTTT
22. Pre-eclampsia is recognised to be associated with: a) Hyperplacentosis b) Hyperuricaemia c) Grand multiparity d) Thrombocytosis e) Cigarette smoking TTFFF 23. The following pregnancy complications are recognised associations with diabetes mellitus: a) Pre-eclampsia b) Shoulder dystocia c) Hyperemesis gravidarum d) Polyhydramnios e) Neonatal hypoglycaemia TTFTT
24. Iron deficiency anaemia during pregnancy is associated with: a) multiple pregnancy b) high parity c) high mean cell volume d) low socio-economic group e) Rhesus isoimmunisation 25. Concerning breech presentation: a) The incidence of breech presentation is increased in pre-term (compared with term) labour b) Breech presentation is associated with an increased incidence of fetal abnormality c) Breech presentation is associated with uterine abnormality d) Lovset manoeuvre may be used to assist the delivery e) Breech extraction is associated with an increased risk of intra-abdominal haemorrhage in the neonate TTFTF TTTTT
26. The following precautions should be taken before Caesarean Section: a) Antacids should be given to the mother b) Urinary bladder should be emptied c) The patient should be lying flat on her back d) The patient should be consented for hysterectomy e) Forceps should be ready for use if needed TTFFT 27. The following features may be associated with fetal hypoxia/acidosis in labour: a) Meconium stained liquor b) Fetal heart rate of 140 beats per minute c) Fetal heart decelerations after contractions d) Fetal heart decelerations with contractions e) Fetal scalp blood pH of > 7.25 TFTFF
28. The following features are characteristically associated with placenta Praevia: a) Painless antepartum haemorrhage b) Shock compatible with revealed blood loss c) Fetal intrauterine growth restriction d) Oblique lie e) Pregnancy induced (gestational) hypertension TTFTF 29. Factors associated with an increased risk of fetal abnormality include: a) Repeated ultrasonic examination of pregnancy b) Previous obstetric history of an infant with a neural tube defect c) Maternal diabetes mellitus d) Maternal age greater than 40 years e) Family history of age-related Down’s syndrome FTTTF
30. The following statements relate to engagement of the presenting part: a) It is defined as the passage of the widest diameter of the presenting part through the plane of the pelvic inlet b) In an engaged cephalic presentation less than two fifths of the head is palpable abdominally c) The occiput of the completely engaged head can be felt vaginally above the level of the ischial spines d) Forceps can only be applied if the head is engaged e) Elective caesarean section is indicated if the presenting part is not engaged at term TTFTF